Background:
Permanent pacing in patients with severe tricuspid regurgitation (TR) and marked atrial enlargement remains technically demanding. Transvenous leads can worsen TR, interfere with future valve interventions, and increase the risk of bleeding or infection in multimorbid patients. Leadless pacemakers have emerged as a valuable alternative, yet implantation may be challenging in patients with distorted right-heart anatomy.
Case summary:
A 75-year-old man with permanent atrial fibrillation, previous mitral valve repair, and severe secondary TR was admitted with cardiac decompensation and symptomatic bradycardia. Echocardiography revealed extreme biatrial enlargement (left atrial volume 2755 mL, right atrial volume 557 mL) with compression of the right atrium and ventricle (Figure 1). Leadless pacing (Micra™, Medtronic) was chosen due to several reasons: the complex anatomy, high bleeding and infectious risk because of comorbidities and need for future surgical valve repair.
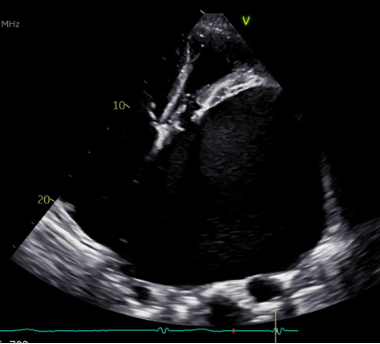
Figure 1:transthoracic echocardiography showing massive biatrial dilatation
The transjugular route provided superior catheter control and facilitated septal positioning within the markedly dilated right heart. Correct septal contact was verified by the fluoroscopic “flamingo-neck” configuration (Figure 2) and contrast injection. Despite multiple repositioning attempts, implantation was successfully completed without complications. Pacing thresholds were stable, and the patient was discharged two days later in good clinical condition. A subsequent methicillin-sensitive Staphylococcus aureus bacteremia was unrelated to the device.
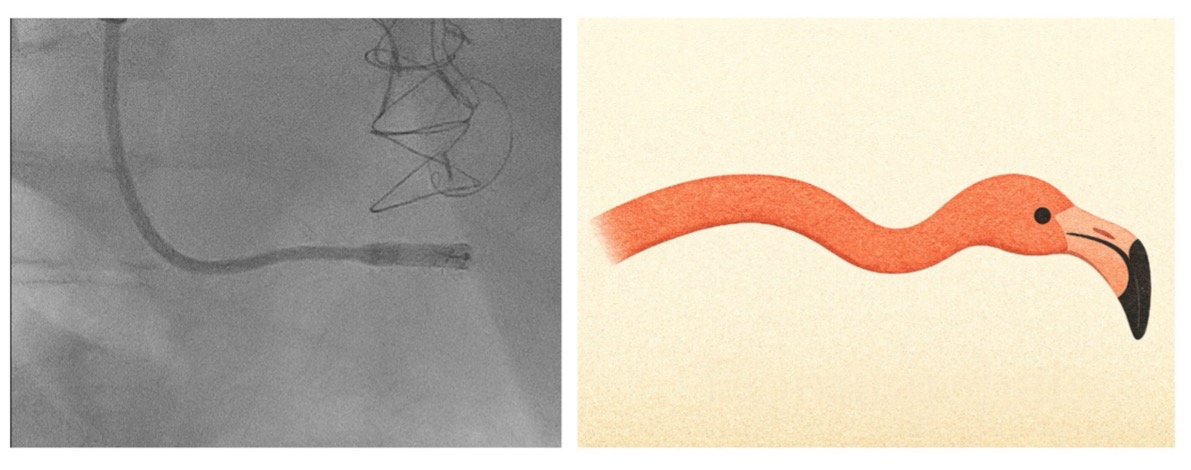
Figure 2: lef: Fluoroscopic image: leadless pacemaker delivery catheter in the right ventricle; right: schematic illustration of “flamingo-neck” configuration during septal positioning (generated by OpenAI, 2025)
Discussion
In this patient with massive biatrial dilation and severe TR, standard transfemoral access would have limited catheter maneuverability and increased the risk of apical placement or perforation. The transjugular approach allowed a more controlled trajectory toward the interventricular septum and may reduce vascular complications. This case illustrates the procedural feasibility of leadless pacing in anatomically extreme conditions and supports individualized access strategies in complex structural heart disease. Conclusion:
Transjugular leadless pacemaker implantation is a safe and effective alternative to transfemoral access in patients with massive atrial dilation and severe TR. This technique offers improved catheter control, facilitates septal fixation, and preserves future tricuspid valve intervention options.



