Background: Mitral transcatheter edge-to-edge repair (M-TEER) is an established treatment for severe mitral regurgitation (MR). Despite procedural advances, mortality remains high. Therefore, we aimed to investigate whether residual MR and clinical factors independently predict one-year all-cause mortality (ACM) after M-TEER.
Methods and results: This is a retrospective, observational, multicentre study. We enrolled 1644 patients, who were treated with the Abbott MitraClip™ and Edwards PASCAL™ systems between 2010 and 2023 at the university hospitals of Tübingen and Ulm. All patients were followed for 360 days post-procedure. The primary outcome was all-cause mortality.
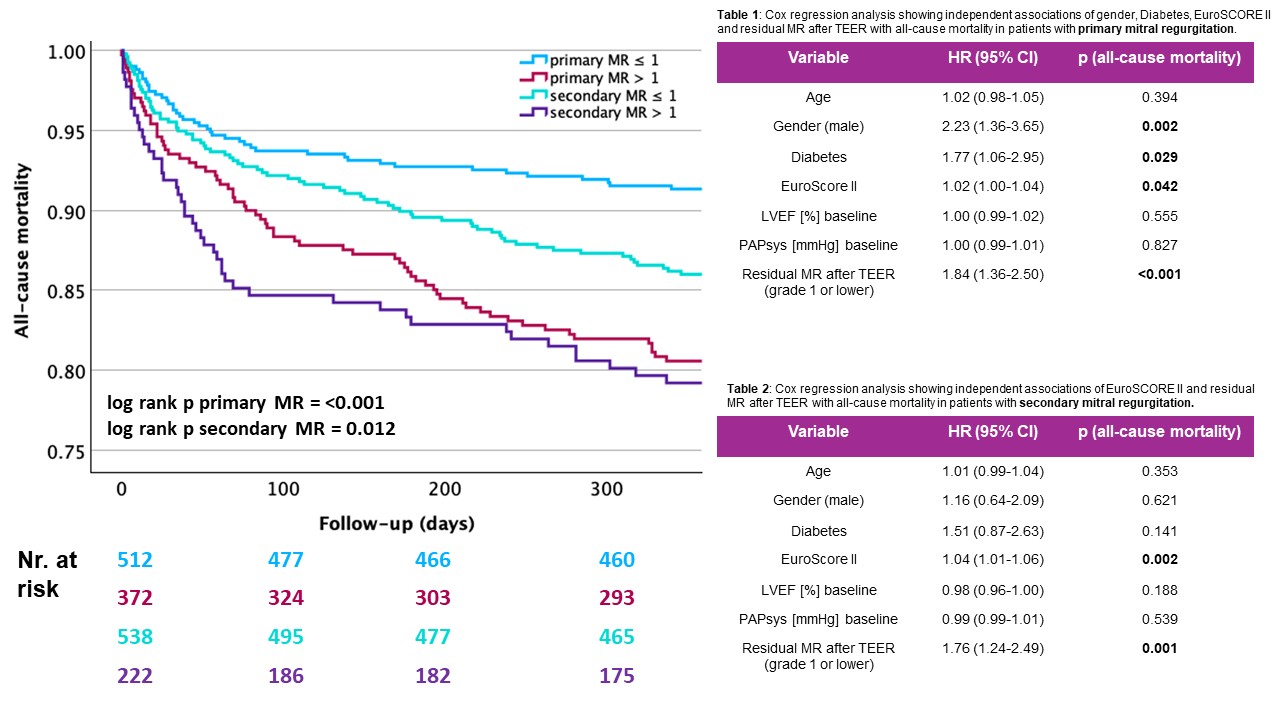
Kaplan-Meier analysis demonstrated that in primary MR, patients with residual MR≤1 had significantly better survival compared to those with residual MR > 1 (p<0.001). In secondary MR, the difference remained statistically significant but was less pronounced (p=0.012). Overall, patients with primary MR showed lower one-year mortality compared to those with secondary MR when stratified by the same post-procedural MR grade.
Multivariable Cox regression confirmed residual MR > 1 to be an independent predictor for one-year mortality in both aetiologies (p<0.001 for primary MR and p=0.001 for secondary MR). In primary MR, male gender (p=0.002), diabetes (p=0.029) and EuroScore II (p=0.042) were associated with higher mortality. In secondary MR (Table 2), EuroScore II also was independently associated with mortality. Age, baseline left ventricular ejection fraction and baseline systolic pulmonary artery pressure showed no significant effect in both groups.
Conclusion: The current study demonstrates that residual MR > 1 after M-TEER significantly increases the risk of one-year mortality risk in both primary and secondary MR patients. Alongside clinical factors like gender and EuroSCORE II, residual MR is a key determinant of patient prognosis. Patients with primary MR show overall better survival than those with secondary MR. Optimizing procedural success to minimize residual MR may substantially improve outcomes in this high-risk population.