Background
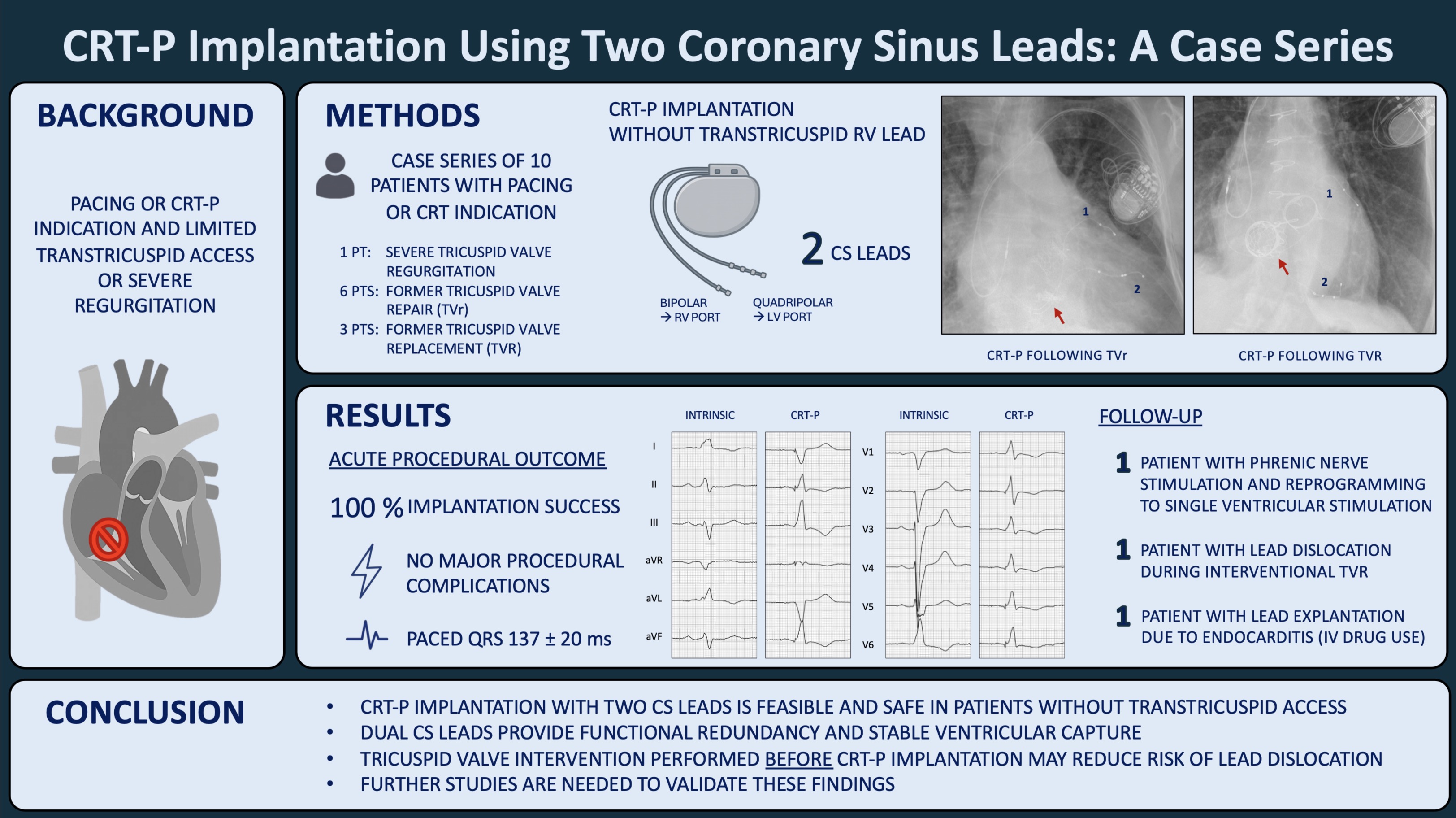
The number of tricuspid valve (TV) interventions is increasing rapidly, driven by greater awareness of tricuspid regurgitation (TR) and the emergence of novel transcatheter techniques and devices. Many patients with prior or planned TV interventions require pacing or cardiac resynchronization therapy. Conventional right ventricular (RV) leads may exacerbate TR or be challenging to implant after such interventions.
Aim
The aim of this case series was to report procedural data and outcomes of patients with cardiac resynchronization therapy pacemaker (CRT-P) implantation using two coronary sinus (CS) leads instead of a conventional RV lead.
Methods
All de novo CRT-P implantations using two CS leads performed at our center between 2022 and 2025 were included. A bipolar CS lead was connected to the RV port and a quadripolar CS lead to the LV port. Procedural success, complications and follow-up parameters were analyzed retrospectively.
Results
A total of ten patients (70.1 ± 22.2y; 60% male) underwent CRT-P implantation with two CS leads. Cardiac resynchronization therapy was indicated in two patients and pacing in nine (4 total heart block; 3 atrial fibrillation with slow ventricular response; 2 sick sinus syndrome/sinus bradycardia) with one patient meeting both indications. Nine patients had undergone prior surgical (2 TVR (bio), 1 reconstruction) and/or transcatheter (6 T-TEER, 1 Evoque) TV procedures and one patient presented with severe TR and pacemaker-associated cardiomyopathy. CRT-P implantation was successful in all cases and no major periprocedural complications occurred. The mean paced QRS duration was 137 20ms. Median follow-up duration was 345 days. In all patients, lead parameters were stable and in both patients with an indication for resynchronization biventricular stimulation was ≥ 97%. There was no significant change in mean LVEF (51 ± 9% vs. 52 ± 9%; p = 0.894). One patient experienced phrenic nerve stimulation in all vectors of the quadripolar CS lead, requiring reprogramming to single-ventricular pacing. Furthermore, two devices maintained an appropriate function but were explanted: In one patient, interventional TV replacement led to lead dislocation of the CS leads requiring revision. In the other case, recurrent endocarditis related to continued intravenous drug abuse after TV replacement necessitated repeat surgery and complete system explantation.
Conclusion
This case series provides initial evidence that CRT-P implantation with two CS leads might be a feasible and safe pacing alternative for patients in whom trans-tricuspid access is contraindicated or not possible. Placing two CS leads offers functional redundancy, potentially lowering the risk of lead failure and loss of ventricular capture. TV intervention performed prior to pacemaker implantation, rather than afterwards, may help minimize the risk of lead dislocation in this patient population. Larger prospective studies are needed to confirm these results.