Background: Mechanical cardiopulmonary resuscitation (mCPR) using dedicated chest compression systems was developed to ensure the quality of chest compressions and to enhance the safety of emergency medical services (EMS) personnel during transport while resuscitation is ongoing. However, these systems are also used outside of patient transport. Only a few studies have investigated the effects of these mCPR devices on patient outcomes.
Methods: We aimed to evaluate the clinical outcomes of patients who were treated with mCPR devices after out-of-hospital cardiac arrest (OHCA).
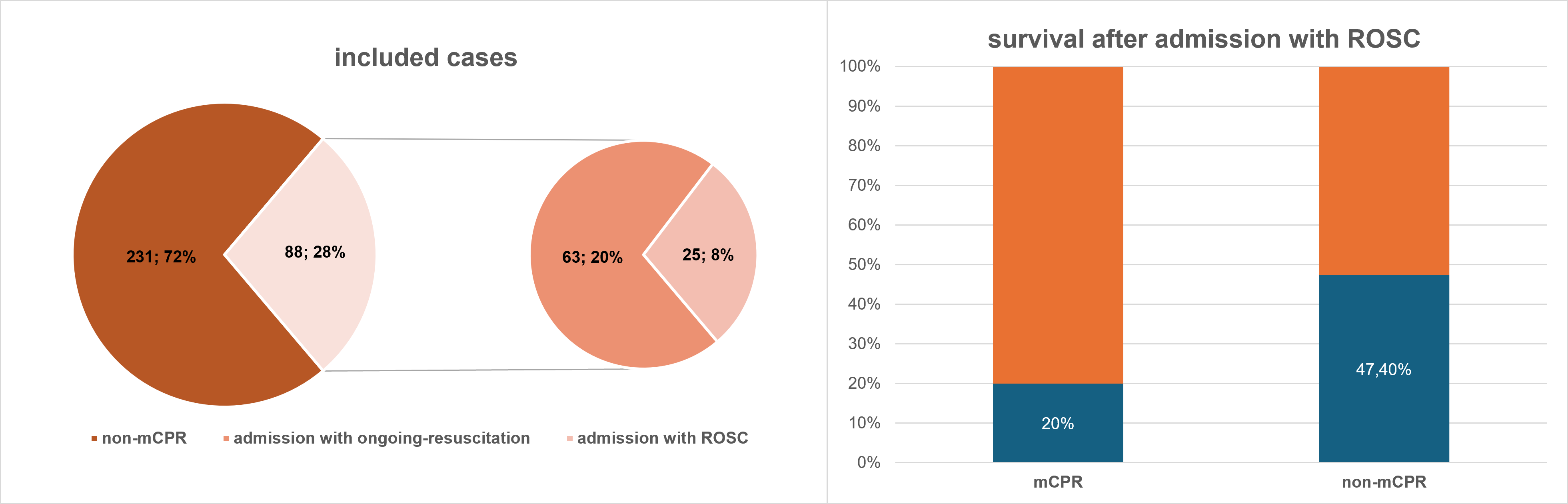
Results: This single-centre retrospective observational study included 319 cases of OHCA transferred to our hospital between 1 January 2020 and 31 March 2025. All patients were transported by EMS either during ongoing resuscitation or after return of spontaneous circulation (ROSC). mCPR was used in 88 cases, 63 of whom arrived at the hospital under ongoing resuscitation. The mean patient age was 66.4 years and 76.5% were male. The causes of cardiac arrest were acute coronary syndrome in 33.0% of cases, pulmonary embolism in 4.2%, non-medical causes in 9.1%, and unknown causes in 23.1%. The mean duration of resuscitation was 29 minutes, 54 minutes in cases where mCPR was used and 15 minutes without mCPR. Bystander CPR was performed in 69.9% cases, and in 62.5% the collapse was witnessed with immediate initiation of resuscitation. In 47.5% of cases, the initial rhythm was ventricular fibrillation, in 29.7% asystole, in 19.6% PEA, and in 3.3% it was unknown. Extracorporeal life support (ECLS) was performed in 12 cases. Among all patients with OHCA, 64.9% died, with 43.0% of deaths occurring on the day of admission. Among survivors, 91.0% achieved a good neurological outcome (CPC ≤2) at discharge. Of the 63 patients admitted under ongoing mCPR, mortality was 95.2%. ECLS was initiated only in 7 patients (11.1%) admitted with mCPR, of whom two survived. All surviving mCPR patients had a CPC score of 1 at discharge. A total 25 patients treated with mCPR were admitted with ROSC. Of these, 80% died compared to 52.6% of patients without mCPR. Imaging (X-ray or CT) revealed trauma-related findings in 72.8% of cases. Following mCPR, sternal fractures (39.1% vs. 19.0%) and pre-/retrosternal hematomas (33.3% vs. 6.1%) occurred significantly more frequently than in patients without mCPR.
Conclusion: The survival rate of patients admitted under ongoing resuscitation with mCPR was extremely low (<5%), and only around 11% of these patients received ECLS. These findings indicate suboptimal prehospital selection of patients for transport under mCPR for advanced in-hospital therapies, including ECLS. This warrants optimization of emergency care structures through the establishment of a dedicated eCPR program, including specialized training of emergency personnel, precise communication between pre- and in-hospital teams, and narrowly defined indications for mCPR use. We found an increased incidence of sternal fractures associated with mCPR use, as well as reduced survival rates among patients admitted with ROSC following mCPR compared with those without mCPR. These findings warrant further investigation. As mCPR appears to be more traumatic, its use should be restricted to essential situations, such as transport under ongoing resuscitation.