ABSTRACT
Background: The self-expanding intraannular NAVITOR transcatheter aortic valve was designed to ensure a safe coronary access with ist intraannular design and extra large stent struts. Coronary obstruction (CO) remains a rare but possibly fatal complication. Several studies examined coronary access after transcatheter aortic valve replacement (TAVR), dedicated data on the adjusted NAVITOR device are scarce. Identifying risk factors and optimizing implantation techniques accordingly may be a crucial factor in preventing major cardiac structural complications.
Methods: Between June 2021 and August 2025, 490 patients with severe native aortic valve stenosis were treated with either the NAVITOR (n=387) or NAVITOR Vision (n=103) prosthesis. We screened all patients for known CO risk factors such as low coronary heights, valve-in-valve (VinV) procedures and small sinus of Valsalva (SOV) diameters. To further evaluate the individual mechanisms behind the cases, we retrospectively reviewed each patient with CO.
Results: We identified 84 patients with low coronary distance (< 10 mm; 17,1%). CO occurred in a total of four patients (0,8%). A common factor in all four patients was a low coronary height under 10 mm. In one case, an LCA distance of 9 mm was the only known risk factor. Another patient hat a low coronary height (LCA distance 6 mm) combined with a small SOV diameter. These two cases were not classified as high risk for coronary obstruction preprocedurally. However, in both cases additional device embolization led to CO.
In the other two cases several risk factors were combined: one patient had a low sinotubular junction (STJ) height, a small SOV and STJ diameter, VinV procedure, and low coronary height of both vessels (LCA 5 mm, RCA 4 mm). The last patient presented with CO on day six after TAVI. She was deemed high-risk with a combination of a small SOV diameter, low STJ height and LCA height of 8 mm (see table 1 and 2). All four patients died in-hospital as a result of the CO.
Conclusion: Coronary obstruction is an overall rare complication in TAVR procedures with the NAVITOR device. Our data show either a combination of risk factors or an additional mechanism, especially embolization, contributing to this severe event. Every single CO resulted in death. These cases underline the importance of preprocedural risk assessment as well as the further evaluation of possible safety mechanisms like preemptive coronary wiring.
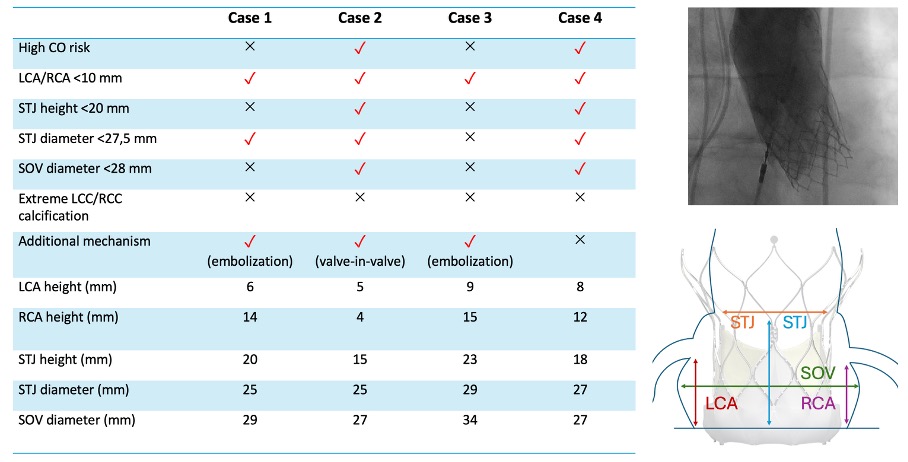
Table 1: Presence of risk factors for coronary obstruction (CO) and individual parameters of each patient. Top right: Aortography showing CO after NAVITOR implantation. Bottom right: Schematic depiction of relevant parameters. Abbreviations: LCA=left coronary artery, RCA=right coronary artery, STJ=sinotubular junction, SOV=sinus of valsalva, LCC=left coronary cusp, RCC=right coronary cusp.
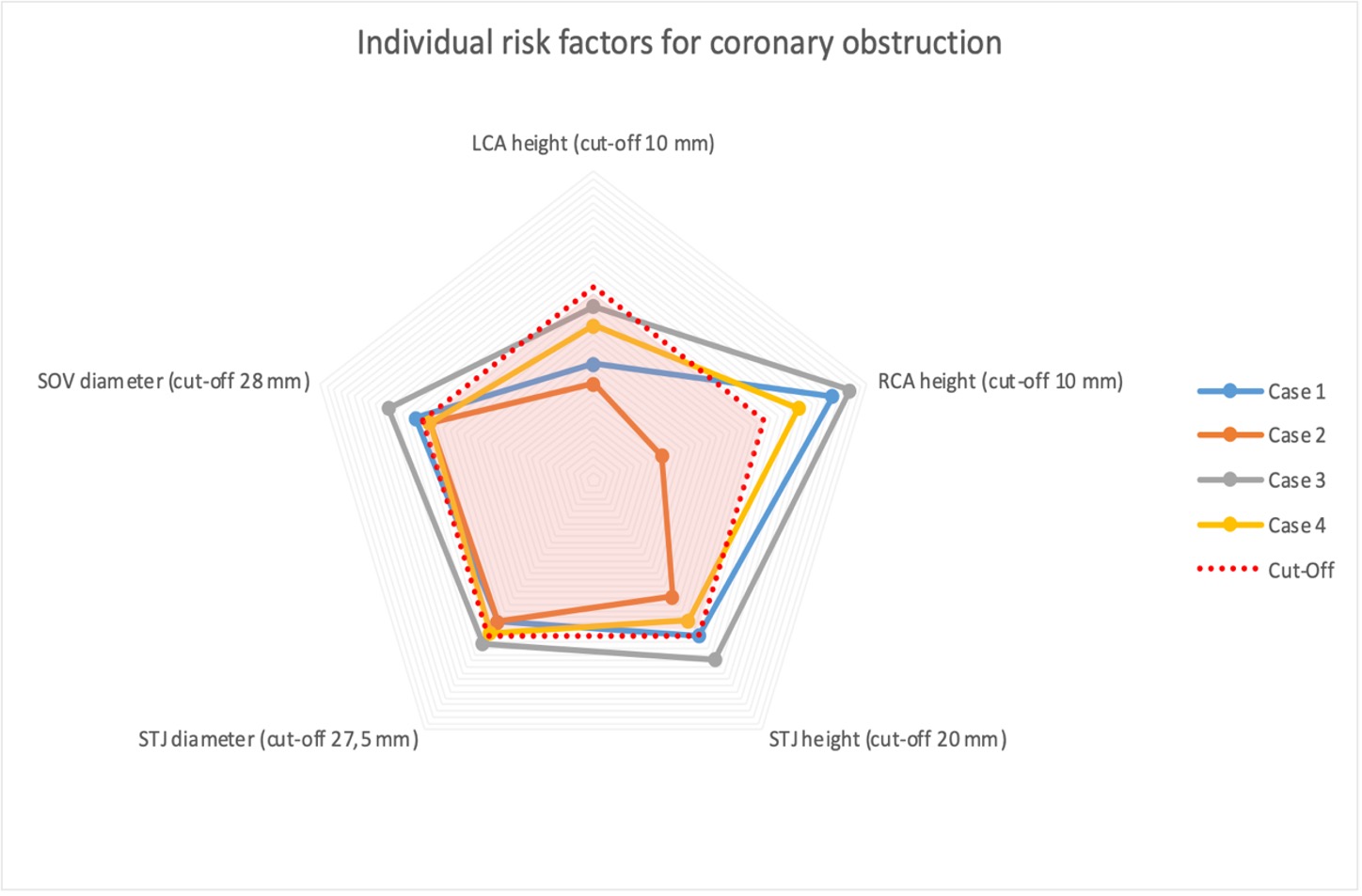
Graph 1: Individual risk factors for coronary obstruction of each patient in relation to the cut-off-value (red area). Abbreviations: LCA=left coronary artery, RCA=right coronary artery, STJ=sinotubular junction, SOV=sinus of valsalva.



