Background: Six years ago, the EAS/ESC guidelines for lipid management in ASCVD patients were put in place. To evaluate the clinical implementation in routine care the LipidSnapshot project was launched as a collaborative approach from industry and physician´s organizations to highlighting the German situation around general practitioners (GPs) and office-based cardiologists (OBCs) in secondary prevention.The aim was to confirm the global finding that especially high-risk patients suffer from a systemic undertreatment in lipid-lowering therapy resulting in a higher risk due to the non-achievement of their respective LDL-C goals.
Methods: Data from ASCVD patients obtained from a prospective, non-interventional multicenter research project with OBCs were compared to patient data from a retrospective, aggregated analysis of anonymous electronic medical records documented by GPs within the IQVIA Disease Analyzer. The proportion of patients reaching pre-defined LDL-C categories, differences in lipid lowering therapies (LLT), gender- and age-related differences in lipoprotein levels as well as LLTs in patients documented by OBCs compared to GPs were assessed in three consecutive years starting 2023.
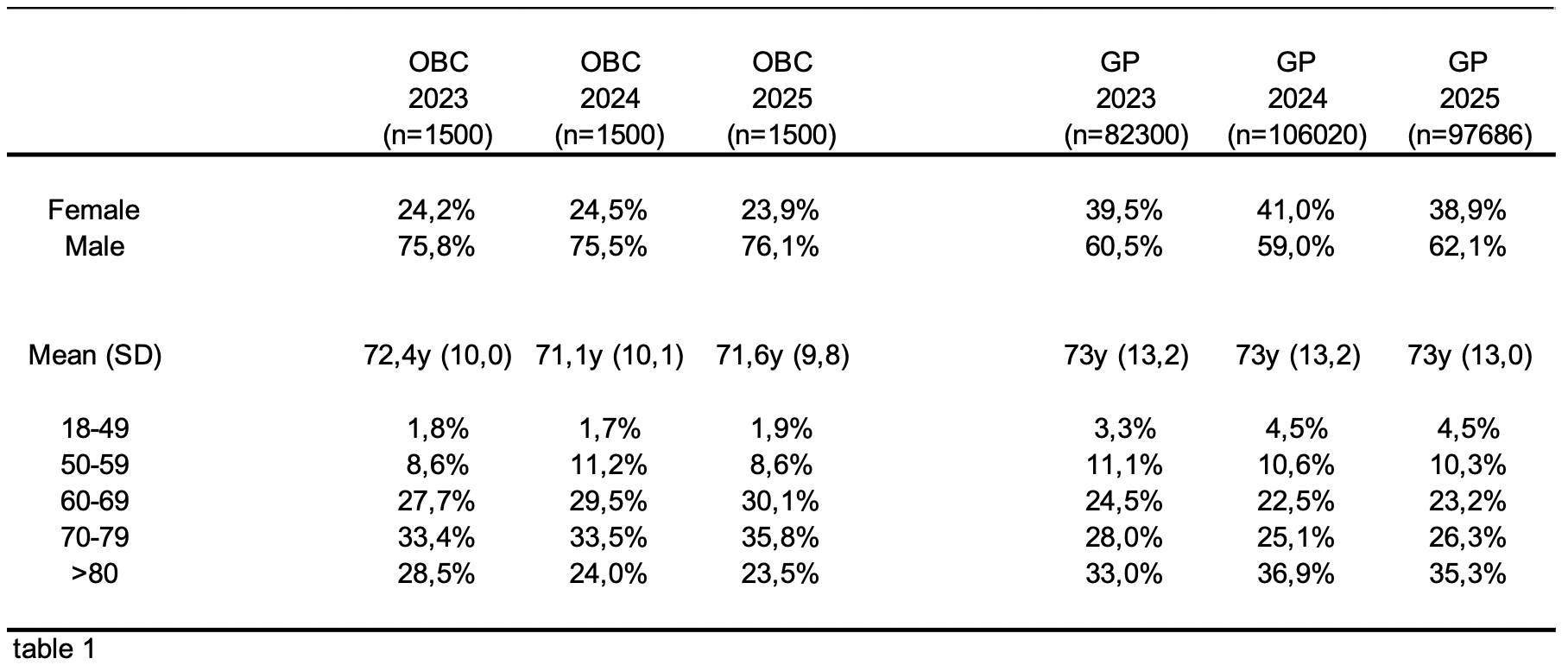
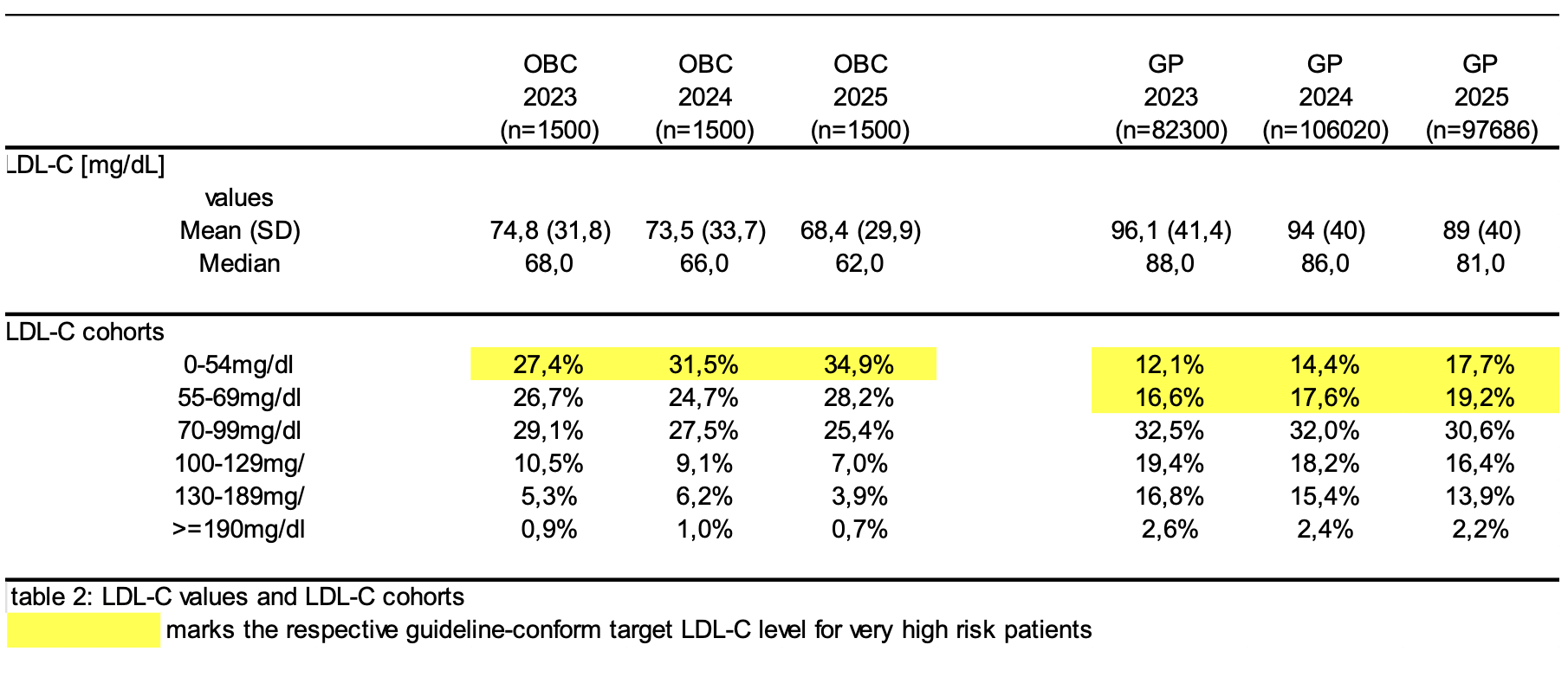
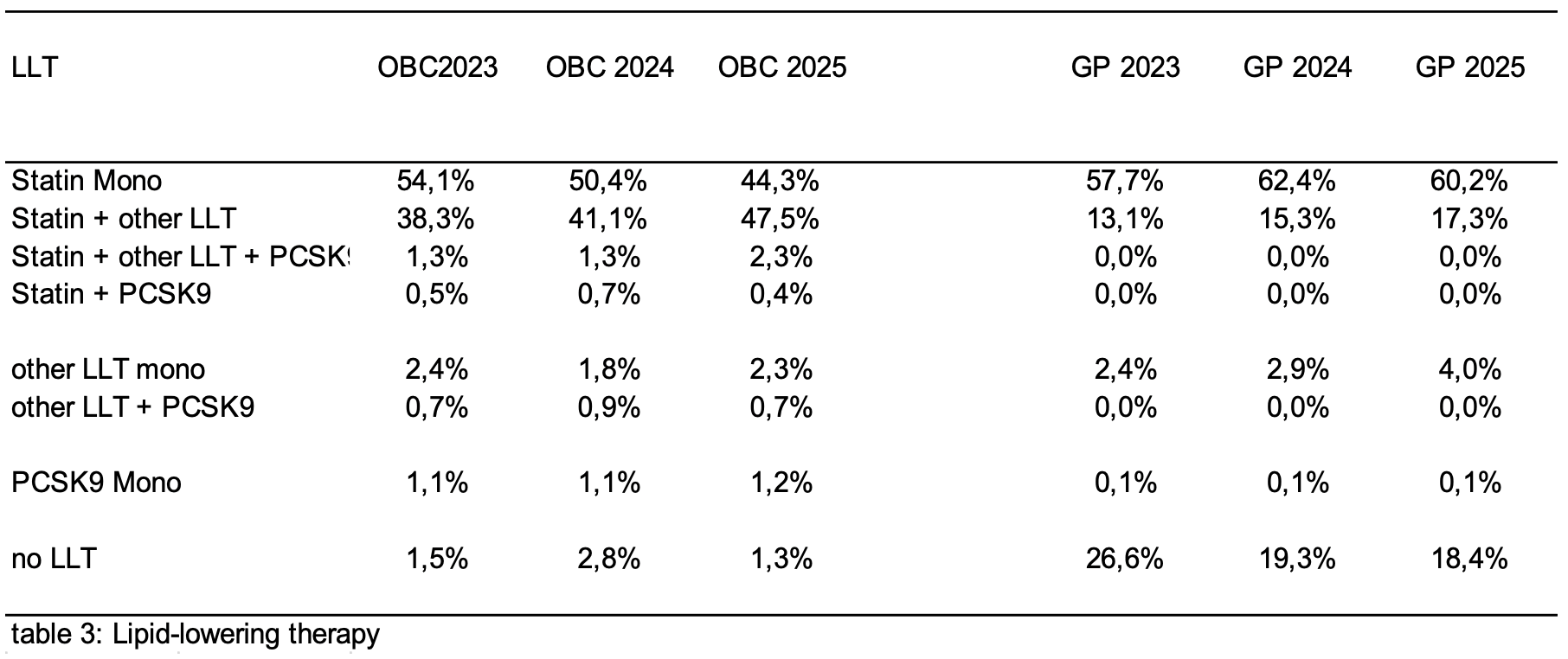
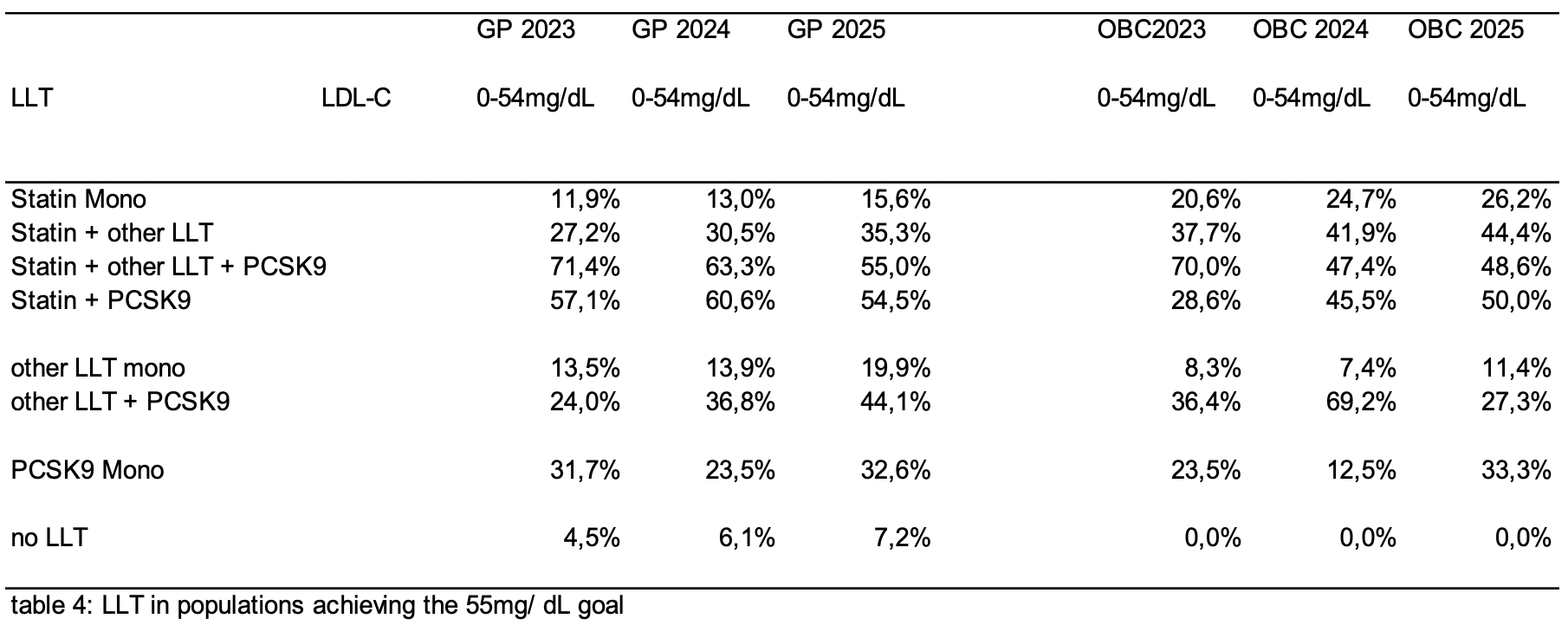
Results: Data from patients at OBCs and patients documented by GPs were included. Mean age at GPs (25% female) between 72.4y to 71.1y and at OBCs (40% female) 73y for all three years, respectively (table 1). With 68.4 mg/dL at OBCs and 89 mg/dL at GPs both current populations show a slightly lower mean LDL-C value compared to the previous years (see table 2 for details). Additionally, the population achieving LDL-C values <55 mg/dL was 34.9% at OBCs compared with 17.7% at GPs, which increased in comparison to the previous years (Table 2). In the current analysis patients of OBCs without any LLT stagnated at 1.3% while patient population without LLT at GPs decreased slightly to 18.4% compared to previous years (table 3). Patient population with statine monotherapy at OBCs is decreasing over the past years to now 44.3% while the patients with statine combination therapy at OBCs is growing in parallel to now 47.5%. All other LLTs are still underrepresented (table 3). With around 60% the vast majority of all patient´s at GPs still receive statine monotherapy. Only 17.3% of the patients receive statine combination therapy which is below the patients receiving no LLT (table 3). Interestingly, in the group of patients achieving the 55mg/ dL LDL-C goal patients with any kind of PCSK9 treatment are overrepresented(table 4).
Conclusion: The majority of ASCVD patients in Germany still do not reach recommended LDL-C target levels. OBCs treat ASCVD patients more often with combined LLT and reach LDL-C targets more often than GPs. Still, one out of five very high-risk patients does not receive any LLT at all from GPs although the numbers a slightly decreasing over the past three years. Additionally, PSCK9 treated patients are more likely to reach LDL-C goals. The data indicate a need to unify guidelines for physicians treating ASCVD patients in Germany.