BACKGROUND
Multivalvular heart disease (MVHD) is prevalent in patients with severe aortic stenosis (AS), with tricuspid regurgitation (TR) being a frequent coexisting condition that increases morbidity and mortality. Traditional management has involved combined surgical aortic valve replacement (SAVR) and tricuspid valve repair (TVR), which, while effective, is associated with higher surgical risk and prolonged recovery. With advances in less invasive techniques, transcatheter aortic valve replacement (TAVR) has emerged as a viable alternative for AS patients. Furthermore, the evolution of transcatheter edge-to-edge repair (TEER) provides a promising option for managing TR. However, comparative data on outcomes between combined SAVR with TVR and TAVR followed by staged TEER remain limited.
OBJECTIVE
The study aimed to evaluate and compare the echocardiographic and clinical outcomes of patients with AS and TR undergoing combined SAVR with TVR versus TAVR with staged TEER.
METHODS
The study included 77 patients with AS and TR treated between 2011 and 2023. Of these, 32 (41.6%) underwent combined SAVR with TVR, while 45 (58.4%) received a TAVR followed by staged TEER. All patients underwent echocardiographic evaluation before the intervention, at discharge, and during follow-up. Clinical endpoints included 30-day and one-year all-cause mortality, as well as VARC-3 defined complications at 30 days.
RESULTS
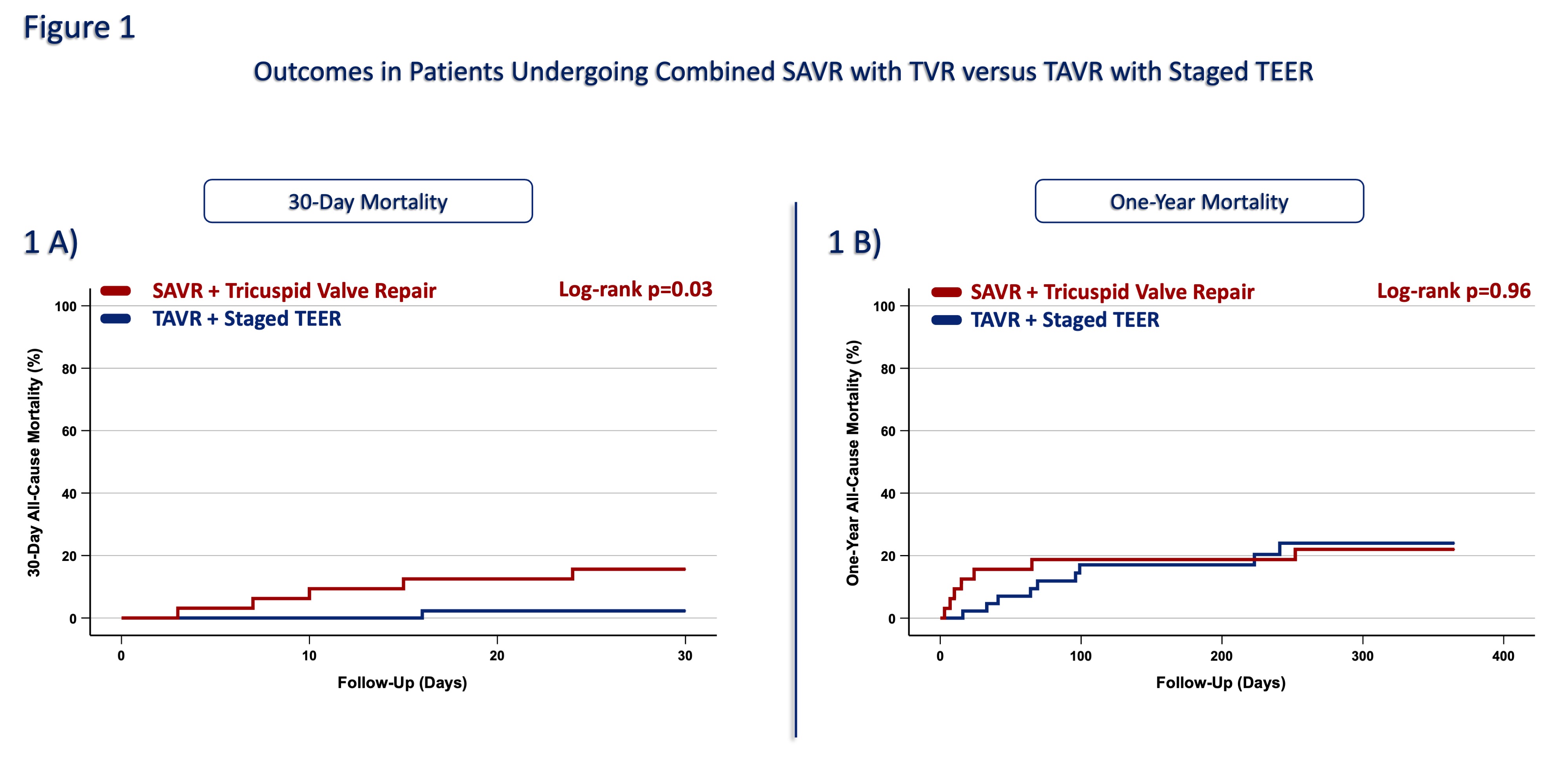
The study population had a mean age of 76.0±10.1 years, with 48.0% being female. The average EuroSCORE II was 5.0%, indicating an intermediate surgical risk in the overall cohort. Patients undergoing SAVR with TVR were significantly younger compared to those treated with TAVR and staged TEER (67.7±9.3 years vs 82.1±5.2 years, p<0.01). Moreover, the SAVR group had a lower surgical risk (EuroSCORE II 5.7% vs 7.2%, p=0.05). The mean left ventricular ejection fraction was 54.5±8.8 %, with no significant difference between both groups (p=0.79). Echocardiographic follow-up demonstrated favorable results across the cohort, with 70.1% of patients showing no/mild residual TR. Moderate residual TR was more frequently observed after staged TEER than surgical repair (20.9% vs 12.5%), though the difference was not statistically significant (p = 0.37). VARC-3-defined complications were comparable between the SAVR and TAVR groups, including acute kidney injury (6.3% vs 5.4%, p=0.57), new pacemaker implantation (9.4% vs 8.9%, p=1.0), and stroke (3.1% vs 0%, p=0.42). The 30-day all-cause mortality was significantly higher in the SAVR with TVR group compared to the TAVR with staged TEER group (15.6% vs 2.2%, p=0.03, Fig 1A). However, the one-year all-cause mortality rates were comparable between both groups (21.9% vs 20%, p=0.96, Fig 1B).
CONCLUSION
In selected patients with AS and concomitant TR, TAVR followed by staged TEER provides comparable clinical and echocardiographic outcomes to combined SAVR with TVR, despite TAVR patients being older and at higher surgical risk. Further studies are warranted to confirm these findings and to refine clinical decision-making in the management of MVHD.