Aim: We sought to identify predictors of peri- and post-interventional bleedings in the 3-year period following TAVR and to compare them to the established factors of a modified version of the PREDICT-TAVR score.
Methods: Data from 1.355 patients undergoing TAVR between 2011 and 2020 were analyzed. Baseline characteristics, cardiovascular risk factors, comorbidities, former procedures, complications and outcomes up to 3-year-follow-up were assessed.
After univariable analysis, variables with p<0.10 were included in a binary logistic regression model. The target variable was the occurrence of bleeding events (BARC 1-5). Taking clinical relevance into account, stepwise forward elimination was performed. The final model was compared to a modified version of the PREDICT-TAVR score (including pre-procedural hemoglobin, oral anticoagulation, post-procedural DAPT and pre-procedural GFR). Modification was necessary due to the data set containing different variables.
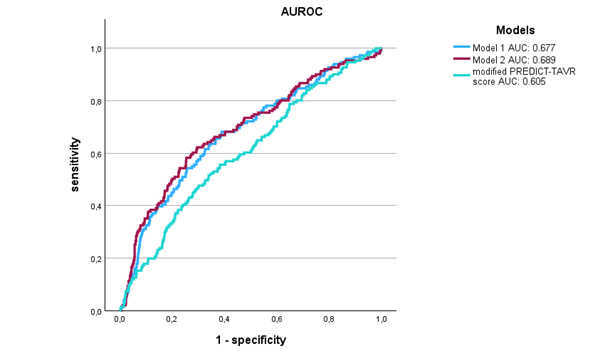
Results: In multivariable analysis, previous bleedings, pre-procedural hemoglobin, pre-procedural platelet count and implant expansion mechanism (ballon-expanding vs. self-expanding) remained significant predictors (see Model 1). Inclusion of pre-procedural GGT (see Model 2) as an additional variable yielded a small but consistent improvement in discrimination (AUC 0.689 vs. 0.677), further exceeding the modified PREDICT-TAVR score (AUC 0.605).
Conclusion: The model showed acceptable discrimination and may support further development of improved bleeding risk scores after TAVR. Unlike the PREDICT-TAVR score, which focuses on 30-day outcomes, our analysis covers 3-year follow-up data, taking into account long-term-bleeding risk after TAVR, emphasizing the relevance of bleeding history and the type of expansion mechanism.



