Background
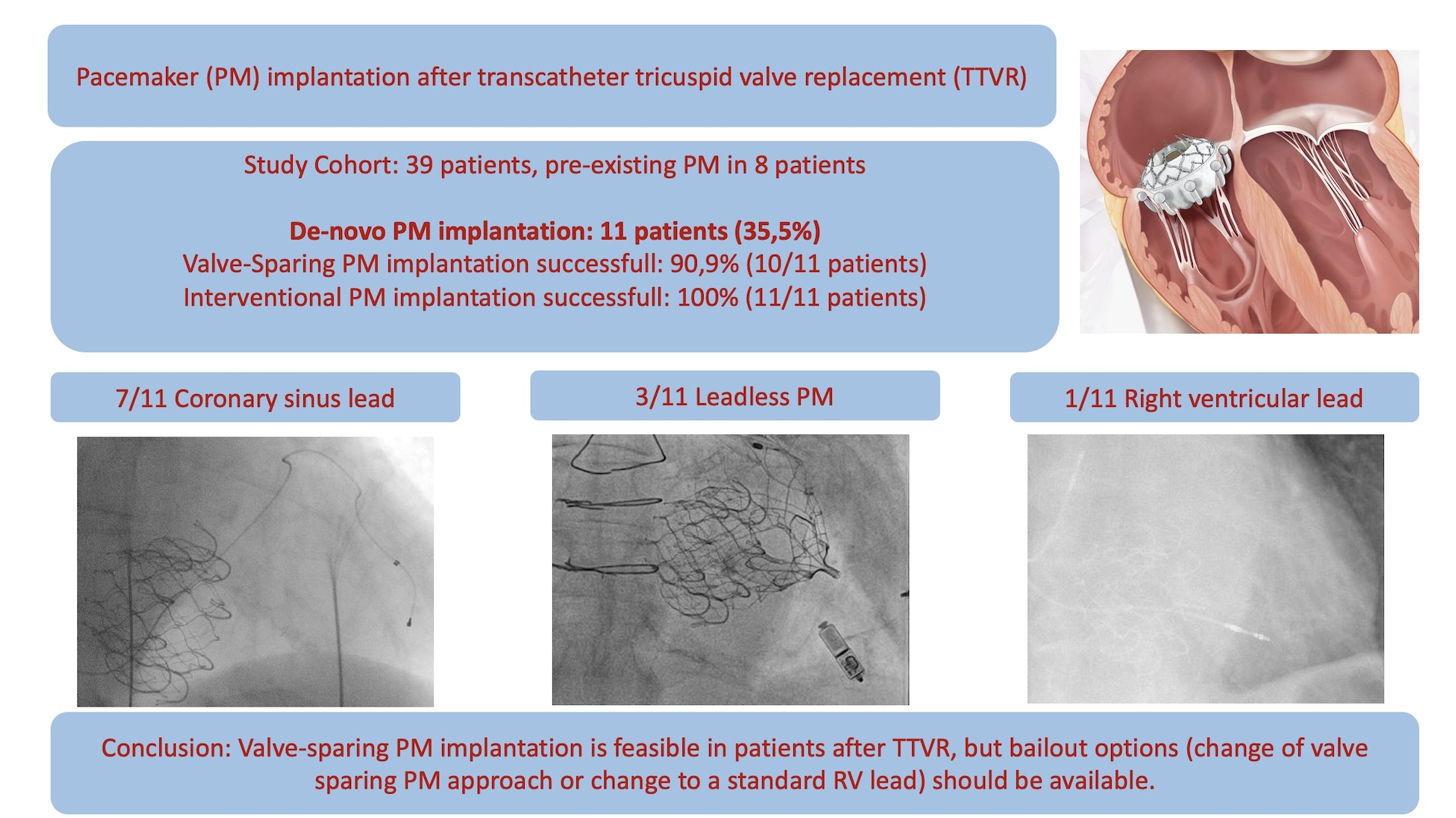
High-degree AV-Block requiring pacemaker (PM) implantation is a frequent complication after transcatheter tricuspid valve replacement (TTVR), which represents a relative contra-indication to standard right ventricular (RV) lead placement. We report our experience in this patient cohort and compared different PM strategies prioritising interventional valve sparing options.
Methods
Consecutive patients treated with the EVOQUE system (Edwards Lifesciences) at our centre between January 2024 and May 2025 were included in this retrospective single centre analysis. Successful implantation of a valve sparing PM and feasibility of PM implantation were assessed.
Results
This analysis included 39 patients (mean age 77.3 years, 74.4% women, 8 patients with pre-existing PM). High-degree AV-Block requiring PM implantation occurred in 28.2% in our cohort (11/39 patients), the de-novo PM implantation rate was 35.5% (11/31 patients). Complete or incomplete right bundle branch block (RBBB) was the most frequent conduction system disorder after TTVR (11/31 patients). Median time from TTVR to PM implantation was six days [IQR: 2.5–13]. PM implantation was feasible in 11/11 patients (100%), no surgical lead placement was necessary. Implantation of a valve sparing PM was successful in 10/11 patients (90.9%). Leadless PM were implanted in 3/11, coronary sinus lead PM in 7/11 patients. In one patient both interventional valve sparing PM approaches failed and a standard RV lead across the EVOQUE system was implanted.
Conclusion
High-degree AV-Block after TTVR is a frequent complication and PM implantation in these patients demands careful consideration. Valve sparing PM approaches appear feasible and were achieved with reasonable success rates in our cohort.