Background: GLP-1 and GLP-2 (glucagon-like peptide-1/2) are incretin hormones which are secreted in the gastrointestinal tract following food intake. GLP-1 and GLP-1 receptor agonists (GLP-1RA) have been extensively studied for their glucose-lowering, weight-reducing and cardioprotective pleiotropic effects, highlighting a mechanistic link in the gut–heart axis. In contrast, GLP-2 does not stimulate insulin secretion, but enhances gut barrier function. In clinical practice, GLP-2RA are indicated in patients with short-bowel syndrome. However, the role of GLP-2 for cardiovascular disease (CVD) is largely unknown.
Methods: Circulating GLP-2 levels were assessed in 539 hospitalized patients which were over the age of 50, fasted and had established atherosclerotic cardiovascular disease (ASCVD). The primary endpoint of this analysis was CV death. Associations of GLP-2 levels with the primary outcome were assessed with Kaplan-Meier curve and uni- and multivariable Cox proportional hazard regression analyses.
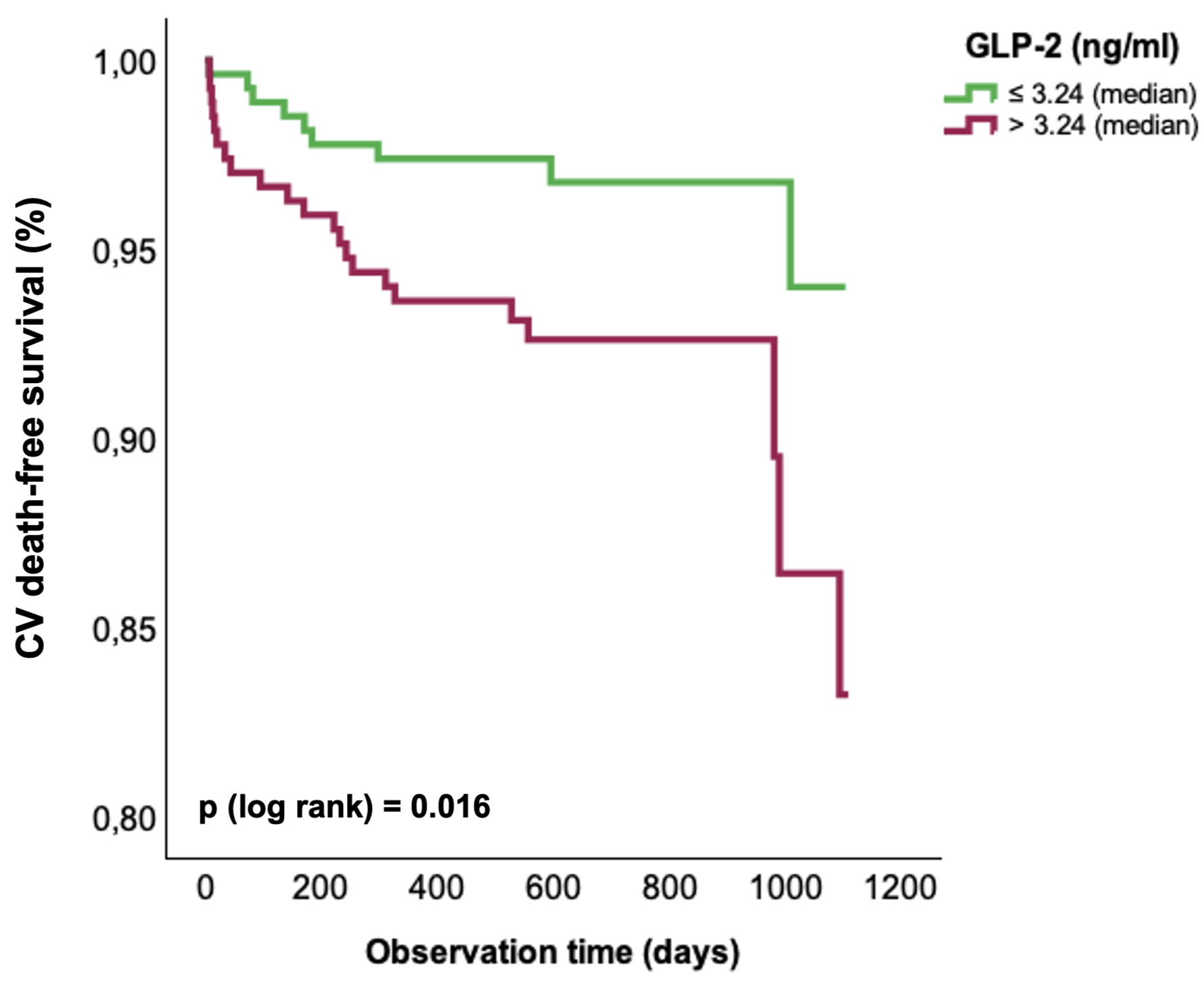
Results: Median GLP-2 levels of the cohort were 3.24 ng/mL. Over a median observation time of two years, CV death occurred in 31 out of 539 subjects. Kaplan Meier curve analyses demonstrated that individuals with GLP-2 levels above the median had a higher rate of CV death than those below the median (log-rank p=0.016). In univariable Cox regression analyses, continuous GLP-2 levels were significantly associated with CV death (Hazard ratio (HR): 1.31; 95% confidence interval (CI): 1.12, 1.52; p<0.001). Moreover, the association between GLP-2 and CV death remained significant in different multivariable models. In model 1 adjusted for age and sex (HR: 1.30; 95% CI: 1.12, 1.52; p<0.001), in model 2 adjusted for low-density lipoprotein cholesterol, high-sensitivity C-reactive protein and lipoprotein (a) (HR: 1.31; 95% CI: 1.12, 1.54; p<0.001) and in model 3 adjusted for N-terminal pro-B-type natriuretic peptide, estimated glomerular filtration rate and total bilirubin (HR: 1.32; 95% CI: 1.13, 1.54; p<0.001) GLP-2 was independently associated with CV death. In model 4, which included standard modifiable risk factors (SMuRF: hypertension, dyslipidemia, type 2 diabetes and smoking) as covariables, this association persisted (HR: 1.20; 95% CI: 1.01, 1.42; p=0.042).
Conclusions: In hospitalized patients with established ASCVD elevated circulating GLP-2 levels were independently associated with CV death. Future studies are needed to investigate whether GLP-2 could be a novel CV risk marker and potential therapeutical target for CVD.