Background: The role of invasively measured pulmonary artery pressure (IPAP) in predicting outcomes among patients with atrial functional mitral regurgitation (AFMR) undergoing transcatheter edge-to-edge mitral valve repair (M-TEER) remains poorly defined.
Aim: To investigate the effect of invasively measured IPAP on the outcomes after M-TEER for AFMR.
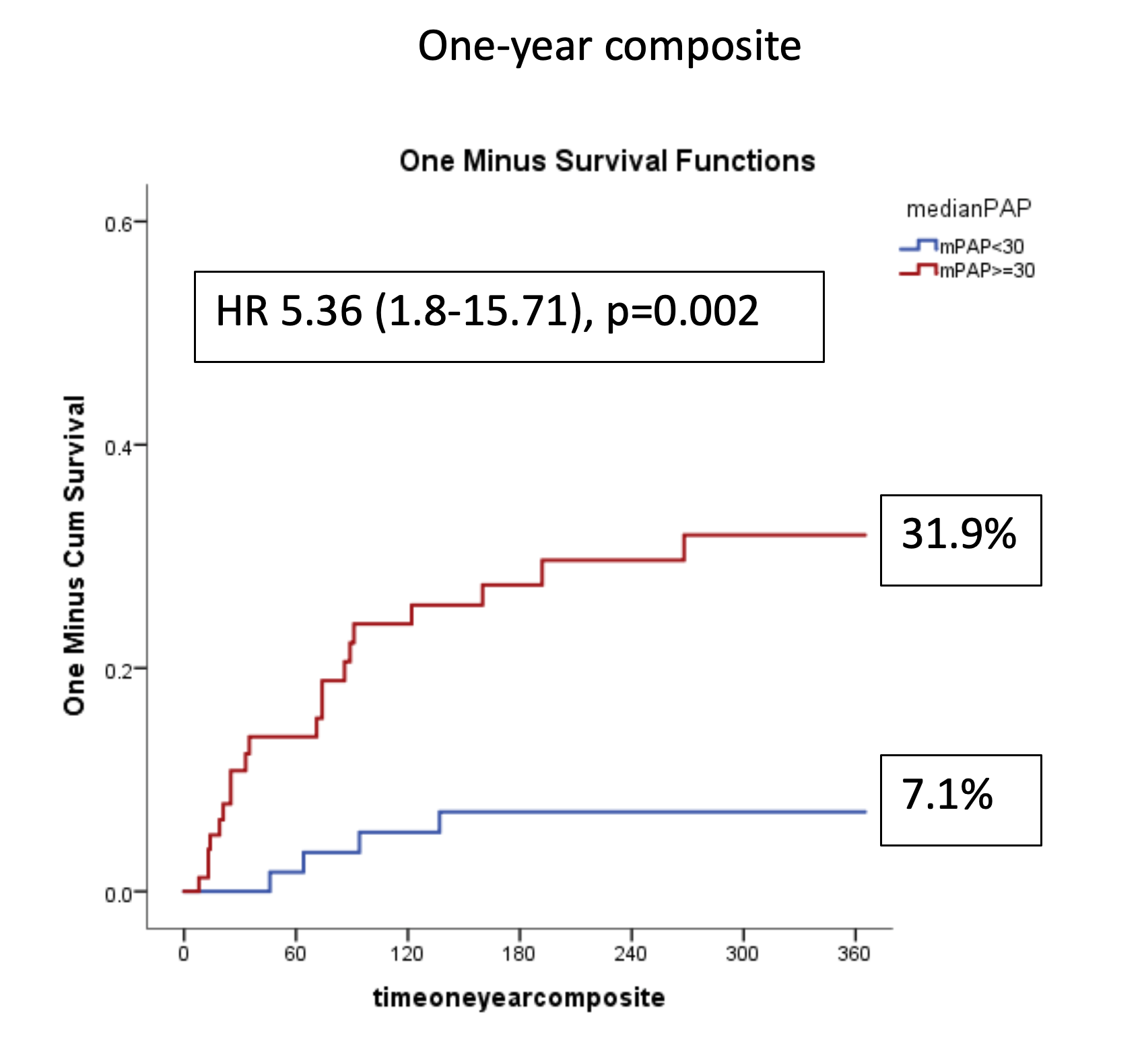
Method: This single-center retrospective analysis included patients with significant mitral regurgitation (MR) treated between 2011 and 2023. Among 727 patients who underwent M-TEER, 179 (24.6%) had AFMR. Invasive hemodynamic measurements were available via right-heart catheterization in 152 of these patients. The cohort was divided according to the median value of invasively measured mean pulmonary artery pressure (PAPm): Group I (low PAPm) with PAPm < 30 mmHg and Group II (high PAPm) with PAPm ≥ 30 mmHg. The primary endpoint was a composite of one-year all-cause mortality and hospitalization due to heart failure.
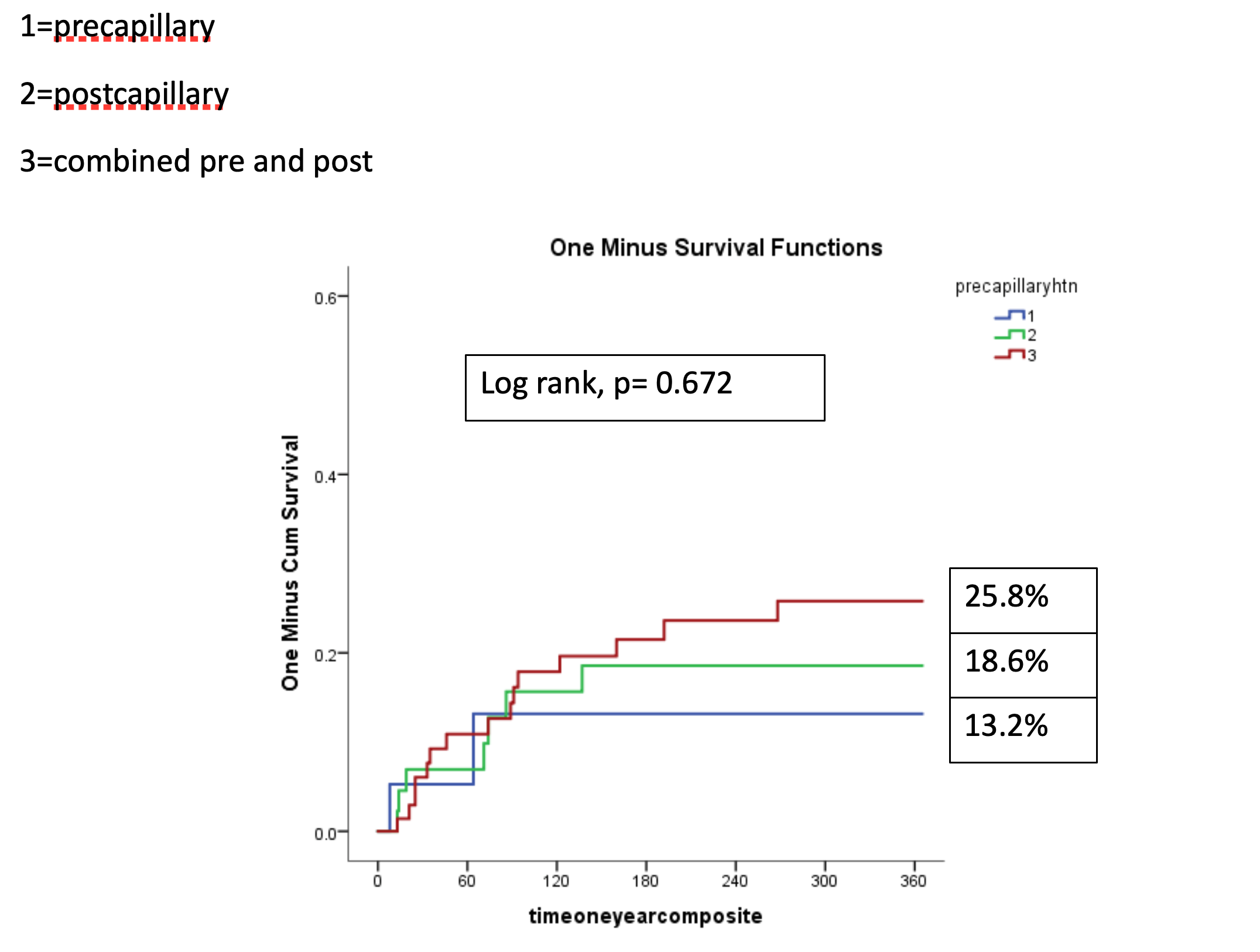
Results: The mean age of the overall cohort was 79.5 ± 6.5 years, and 67.1% were female. Atrial fibrillation was present in 127 patients (83.6%) overall, with a trend toward higher prevalence in the high PAPm group (77.5% vs. 88.9%, p = 0.058). Higher NT-proBNP levels were documented in the high PAPm group (2,415 [1,285–3,415] vs. 3,078 [1,576–5,197] pg/mL, p = 0.054). Combined pre- and post-capillary pulmonary hypertension (PHTN) was the most common subtype among patients with AFMR, followed by post-capillary then pre-capillary PHTN (48%, 29.6% and 12.5% respectively).
A comparable number of clips per patient were implanted in both study groups (p = 0.406). In the overall cohort, procedural success was achieved in 93.9%, with residual MR ≤ 2 observed at close rates in both groups (94.3% vs. 93.7%, p = 0.196).
After one year, patients with higher PAPm had a higher cumulative rate of the composite endpoint (7.1% vs 31.1%, HR 5.36, 95% CI 1.8-15.71, p=0.002). The three subtypes of PHTN (pre-, post-, and combined PHTN) showed no significant differences regarding the composite endpoint (13.2% vs. 18.6% vs. 25.8%, log-rank p = 0.672). Higher invasively measured pulmonary capillary wedge pressure (PCWP) (HR 1.12, 95% CI 1.08–1.18, p < 0.001) and residual MR > 2 after M-TEER (HR 3.46, 95% CI 1.18–10.17, p = 0.024) were associated with more frequent primary endpoint.
Conclusion: In this cohort, AFMR accounted for approximately one-fourth of all MR aetiologies requiring M-TEER. Combined pre- and post-capillary PHTN was the most common subtype among patients with AFMR. Patients with higher invasively measured PAPm had worse one-year outcomes. Additionally, elevated PCWP and residual MR > 2 after M-TEER were independent predictors of adverse outcomes