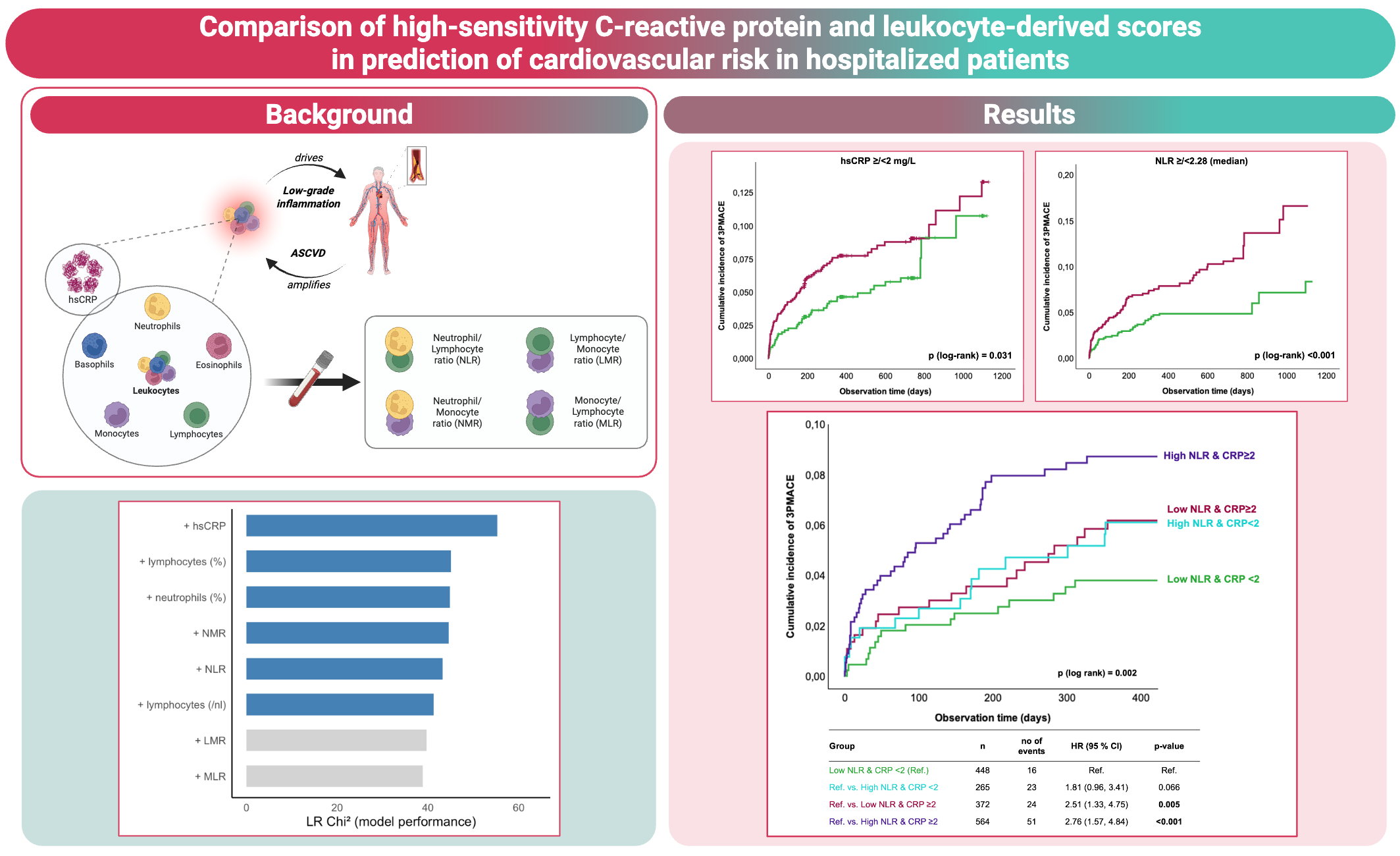
Background: Systemic low-grade inflammation is a key driver of atherosclerotic cardiovascular disease (ASCVD). While high-sensitivity C-reactive protein (hsCRP) is the guideline-recommended biomarker reflecting residual inflammatory risk, the clinical utility of leukocyte-derived scores, such as the neutrophil-to-lymphocyte ratio (NLR) and further indices, remains unclear in hospitalized patients with ASCVD. More information from large, well-characterized cardiovascular (CV) cohorts comparing hsCRP with leukocyte-derived inflammatory indices using contemporary approaches for head-to-head comparison will help clarify their combined clinical utility for risk assessment in high-risk patients.
Methods: In this prospective, single-center cohort study, inflammatory biomarkers including hsCRP, differential leukocyte counts, and leukocyte-derived scores were analyzed in 1649 hospitalized patients. The primary endpoint of this analysis was a composite of non-fatal myocardial infarction, non-fatal stroke and CV death (MACE: major adverse cardiovascular events). Kaplan-Meier and uni- and multivariable Cox regression analyses were performed. Model performance of biomarkers was compared with likelihood ratio Chi2 statistics to assess incremental value for prediction of MACE.
Results: During a median follow-up period of two years, MACE was observed in 114 out of 1649 subjects. Kaplan-Meier curve analyses demonstrated higher incidence of MACE in individuals with hsCRP levels above the guideline-based cut-off of 2 mg/L or those with an NLR above the cohort median of 2.28 (log-rank p (hsCRP) = 0.031; log-rank p (NLR) <0.001). Combined assessment of hsCRP and NLR identified those patients with both markers elevated at highest risk, while risk was intermediate when only one marker was elevated and lowest when both were below the cut-off (log-rank p=0.002). These findings were confirmed in Cox regression analyses showing a 2.8-fold higher risk of MACE in those with high NLR and hsCRP compared with those with low levels of both (Hazard ratio (HR): 2.76; 95% confidence interval (CI): 1.57, 4.84; p<0.001). In further univariable analyses, hsCRP, neutrophil percentage, lymphocyte count and percentage, NLR, neutrophil-to-monocyte ratio (NMR), lymphocyte-to-monocyte ratio (LMR) and monocyte-to-lymphocyte ratio (MLR) were associated with MACE. In multivariable analyses adjusted for age, sex, body mass index, systolic blood pressure, type 2 diabetes, smoking, creatinine, and low-density lipoprotein cholesterol, only hsCRP, neutrophil percentage, lymphocyte percentage, NLR and NMR, but not LMR and MLR, remained independently associated with MACE. In the extended models, hsCRP provided the highest incremental model performance based on likelihood ratio Chi2 statistics, followed by lymphocyte and neutrophil percentages, NMR and NLR, with LMR and MLR contributing least.
Conclusions: In hospitalized patients with high cardiovascular risk, hsCRP and leukocyte-derived indices, particularly NLR and NMR, were independently associated with adverse cardiovascular outcomes. Among all parameters, hsCRP demonstrated the strongest predictive performance, underscoring its role as the most robust established inflammatory biomarker for cardiovascular risk assessment in clinical practice.