BACKGROUND
Concomitant tricuspid regurgitation (TR) is common in patients undergoing TAVI. Previous studies have reported increased mortality in TAVI patients with ≥moderate TR. Emerging evidence suggests that liver dysfunction contributes to adverse outcomes in TR. The Fibrosis-4 (FIB-4) index, a non-invasive marker of hepatic fibrosis, has been associated with adverse outcomes in heart failure and may reflect the hepatic impact of right-sided pressure overload. However, its prognostic value in TAVI patients with persistent TR remains unclear.
OBJECTIVE
We aimed to evaluate the clinical implications of the FIB-4 index in patients undergoing TAVI. Specifically, we sought to assess the predictive value of the index in TAVI patients with ≥moderate TR.
METHODS
The study included 1,797 patients undergoing TAVI. Echocardiography was performed at discharge and at 30-90 days post-procedure to determine the persistence of significant TR despite hemodynamic changes after valve replacement. The patients were stratified into low and high FIB-4 groups based on ROC curve analysis. The primary endpoint was one- and five-year mortality after TAVI.
RESULTS
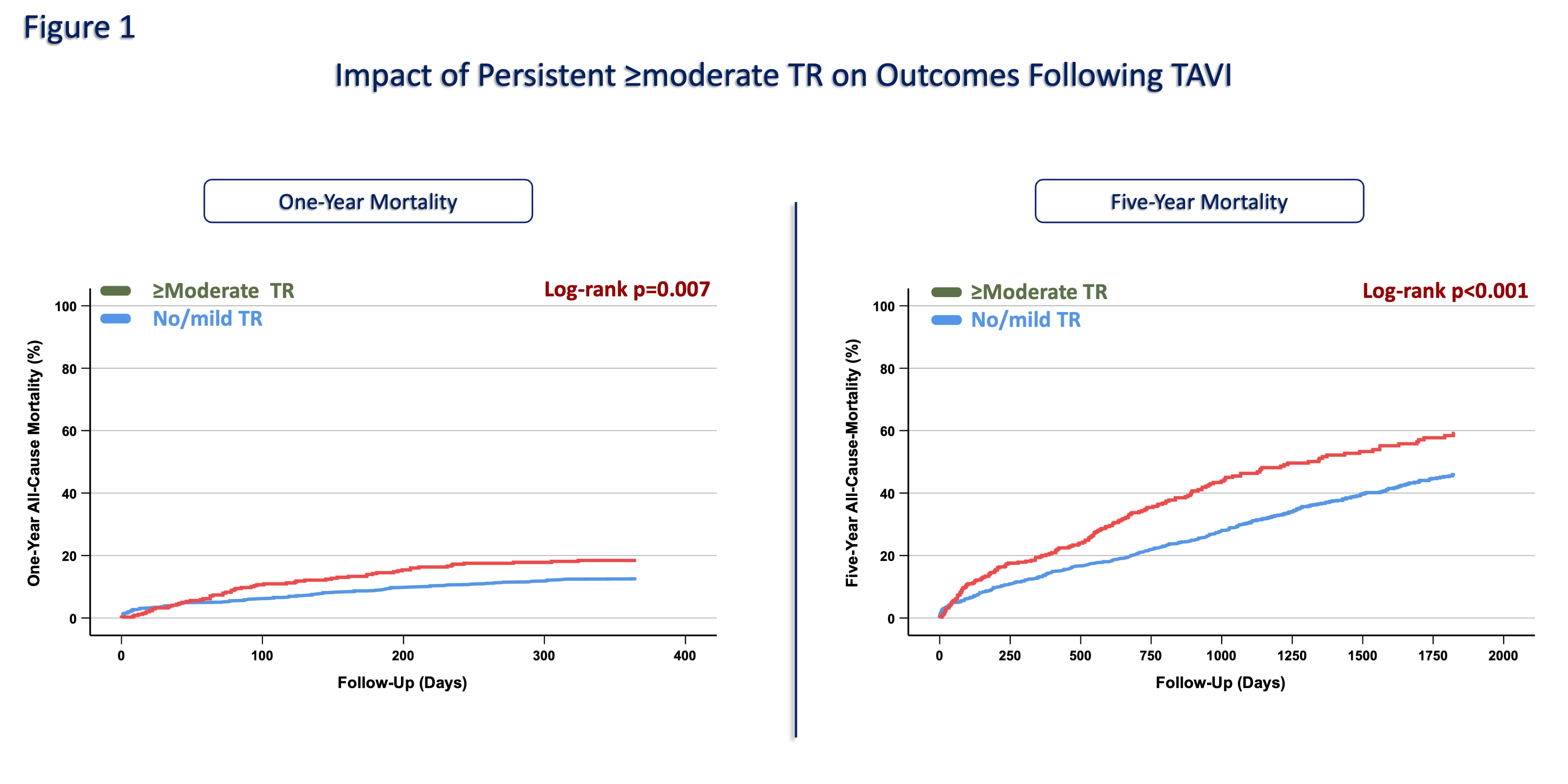
The mean age of the population was 80.9±6.1 years, and 49.5% were female. Concomitant ≥moderate TR was observed in 348 (19.3%) patients. Patients with TR were significantly older (81.9±6.1 vs 80.7±6.0 years, p<0.01) and had lower left ventricular ejection fraction (52.4±12.7 vs 56.4±11.9%, p=0.01). Persistent TR was associated with higher creatinine (1.2 vs 1.1 mg/dL, p<0.01) and troponin levels (32 vs 25 pg/mL, p<0.01). Based on a cutoff value of 1.82, 42.1% of patients with TR were classified as having a low FIB-4 and 57.9% as having a high FIB-4 index. Compared with the low FIB-4 group, patients with a high FIB-4 index had higher rates of pulmonary hypertension (50.2% vs 40.8%, p<0.01), right ventricular dysfunction (37.4% vs 26.9%, p<0.01), and larger inferior vena cava diameter (1.7±0.6 vs 1.3±0.5 cm, p<0.01). One- and five-year mortality was higher in patients with ≥moderate TR compared to those with no/mild TR (17.8% vs 12.3%, p=0.01; 48.4% vs 36.8%, p<0.01, respectively,
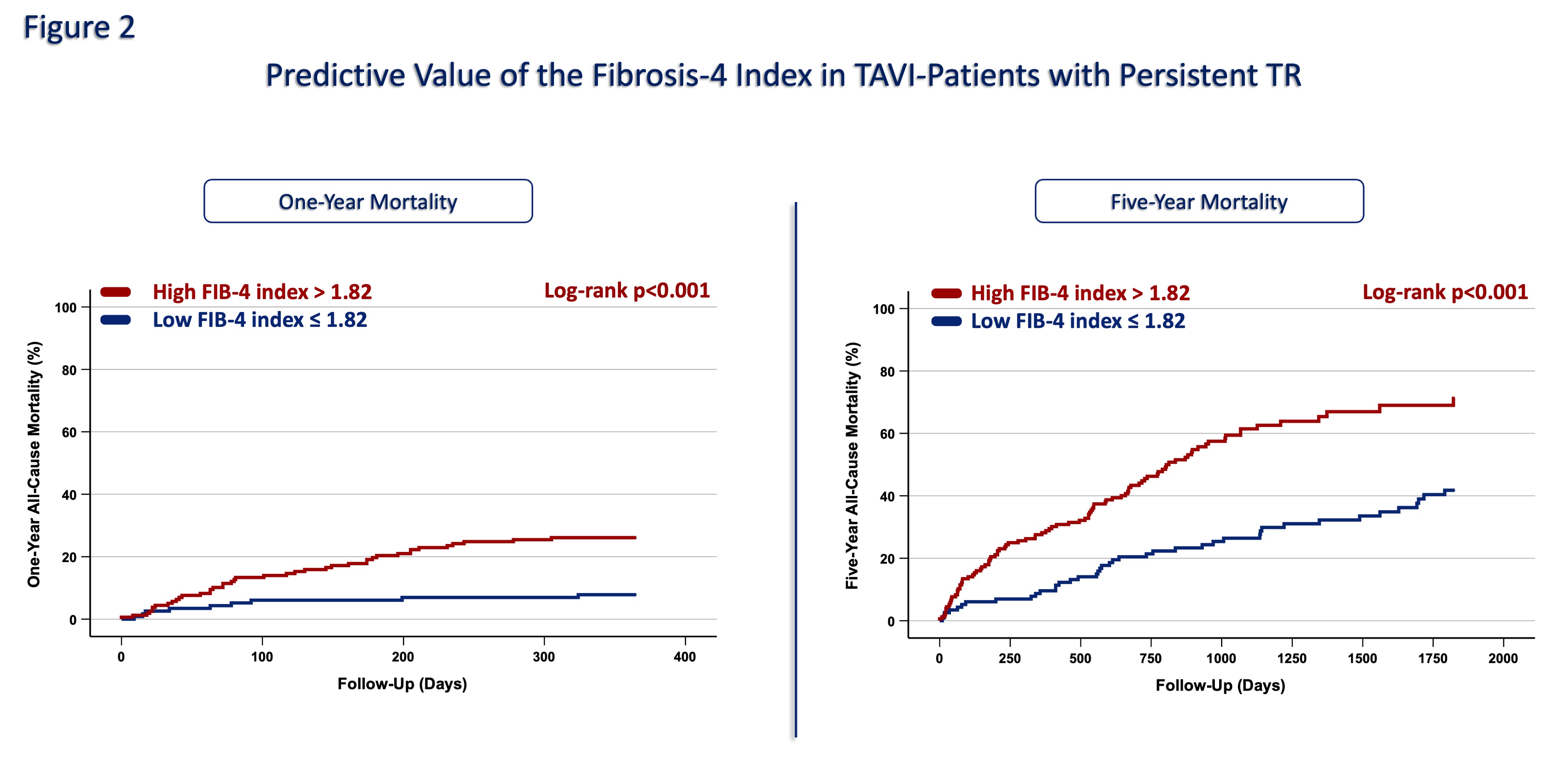
Fig 1). Kaplan-Meier analysis showed that a high FIB-4 index was associated with significantly higher one- and five-year mortality among patients with persistent ≥moderate TR (p<0.01;
Fig 2). Multivariable analysis revealed that a high FIB-4 index was independently associated with mortality in patients with persistent TR (HR: 1.91 [95%CI: 1.07-3.42], p=0.01).
CONCLUSION
In patients undergoing TAVI, persistent ≥moderate TR is associated with adverse outcomes. Among these patients, a high FIB-4 index identifies a subgroup at particularly high mortality risk, independent of other clinical and echocardiographic factors. The index may serve as a useful tool for post-TAVI risk stratification, integrating the impact of hepatic dysfunction into the assessment.