Background: Sleep quality is an important determinant of cardiovascular (CV) health. Poor sleep contributes to adverse CV events through diverse biological mechanisms including sympathetic activation, hormonal dysregulation and low-grade systemic inflammation, but data on the prognostic relevance of sleep quality in hospitalized CV patients remain scarce. More information on the prognostic value of sleep quality, assessed by the Pittsburgh Sleep Quality Index (PSQI), for prediction of adverse outcomes will help clarify its clinical relevance for CV risk assessment.
Methods: Sleep quality was assessed in 1703 patients admitted to a cardiology department using the validated PSQI. The PSQI sum score was categorized according to established cut-offs as good (<5), moderate (5–10) and poor (>10) sleep quality. The primary endpoints were a composite of non-fatal myocardial infarction, non-fatal stroke, or CV death (MACE: major adverse cardiovascular events), all-cause mortality and hospitalization for heart failure (HHF). Associations between PSQI and outcomes were evaluated using Kaplan–Meier curve analyses, uni- and multivariable Cox regression models and variable importance analyses. Model performance was compared with likelihood ratio Chi2 statistics to assess incremental value in risk prediction.
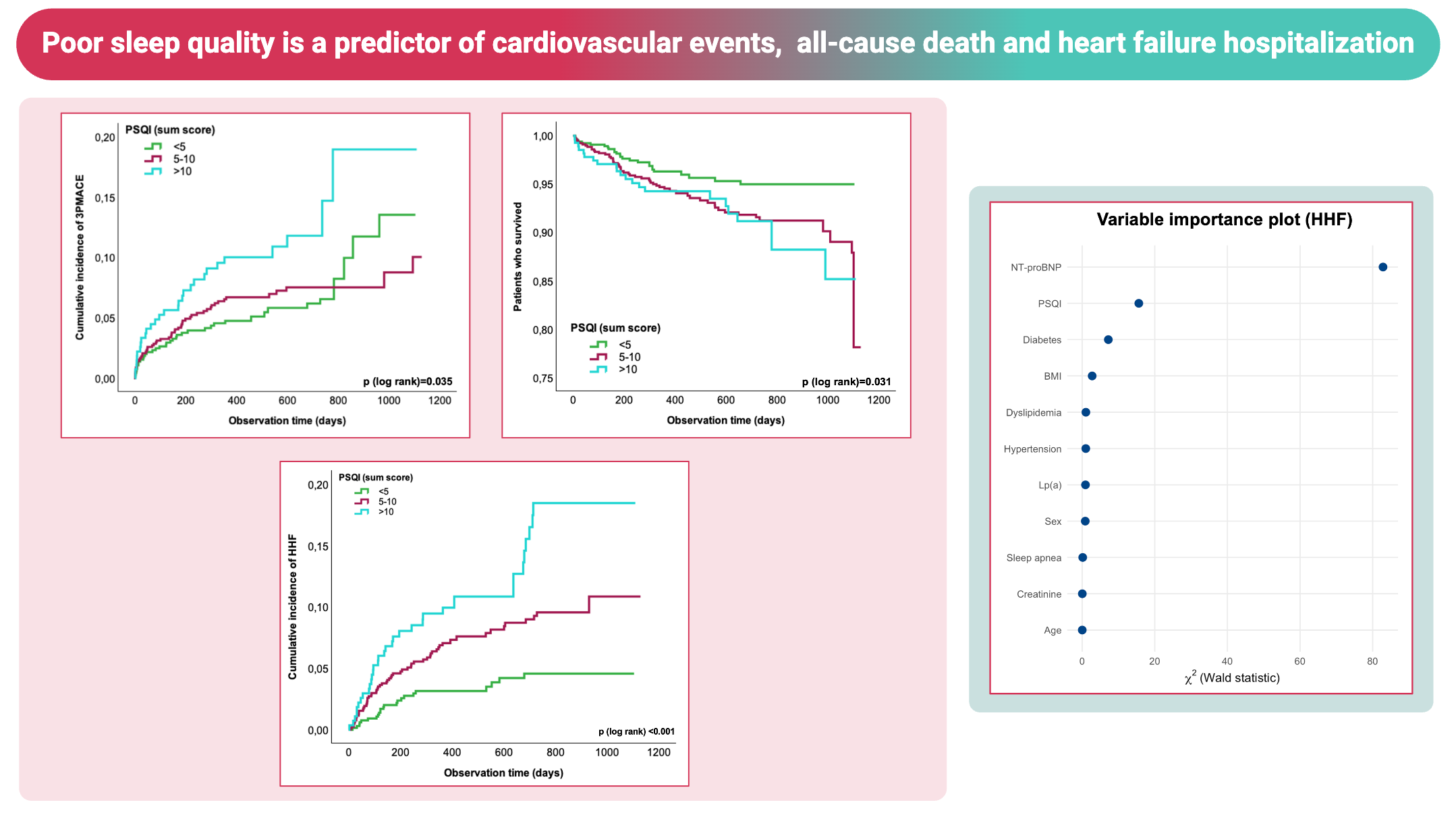
Results: During a median follow-up period of two years, 120 patients experienced MACE, 117 HHF and 104 died. Kaplan–Meier curve analyses showed an increased risk across PSQI categories, with higher scores being associated with higher event rates for MACE (log-rank p=0.035), all-cause death (log-rank p=0.031) and HHF (log-rank p<0.001). Significant differences for HHF were present in subgroups without prior diagnosis of HF (log-rank p=0.016) as well as in those with any history of HF (log-rank p<0.001). Univariable analyses showed a significant association of higher PSQI with MACE (p=0.02), all-cause death (p=0.01) and HHF (p<0.01). These results remained significant after adjustment for age and sex (model 1). With additional adjustment for BMI, hypertension, dyslipidemia, T2DM, sleep apnea, these associations persisted. However, in the fully adjusted model further including N-terminal pro-B-type natriuretic peptide, creatinine and lipoprotein (a) an independent association of PSQI was only observed with HHF, but not with MACE or all-cause death. In model 1 and model 2 PSQI significantly improved overall model performance for prediction of all primary endpoints, while incremental value of PSQI for model 3 was only significant for prediction of HHF (p<0.01), not MACE or all-cause death (p=0.14 and p=0.19). In variable importance analyses based on the contribution of each individual variable from the multivariable model to total risk prediction, PSQI ranked among the strongest predictors of HHF, with only NT-proBNP ranking higher.
Conclusions: In hospitalized patients with CVD, poor sleep quality captured by the PSQI is associated with higher risks of MACE, all-cause death and HHF. After extensive multivariable adjustment, PSQI remained an independent contributor to model performance for prediction of HHF. These findings highlight the importance of sleep quality as a clinically relevant, modifiable lifestyle domain for CV health.