Introduction
Immune checkpoint inhibitor (ICI) associated myocarditis (ICImyocarditis) has been reported to occur in 1% of ICI patients and carries a high mortality up to 50%. Due to the effectiveness of ICIs in cancer treatment, the amount of ICI patients continues to rise. Diagnosing ICImyocarditis early is essential for timely and potentially life-saving immunosuppression. The 2021 International Cardio-Oncology Society (IC-OS) consensus outlines diagnostic criteria. The diagnosis can be made either histologically by a conclusive endomyocardial biopsy (EMB) or based on a significant troponin (Tn) elevation and 1 major or at least 2 minor criteria, including findings of cardiac magnetic resonance imaging (cMRI), electrocardiography (ECG) and others. This case series highlights the diagnostic complexity and expands our understanding of this adverse event.
Case series
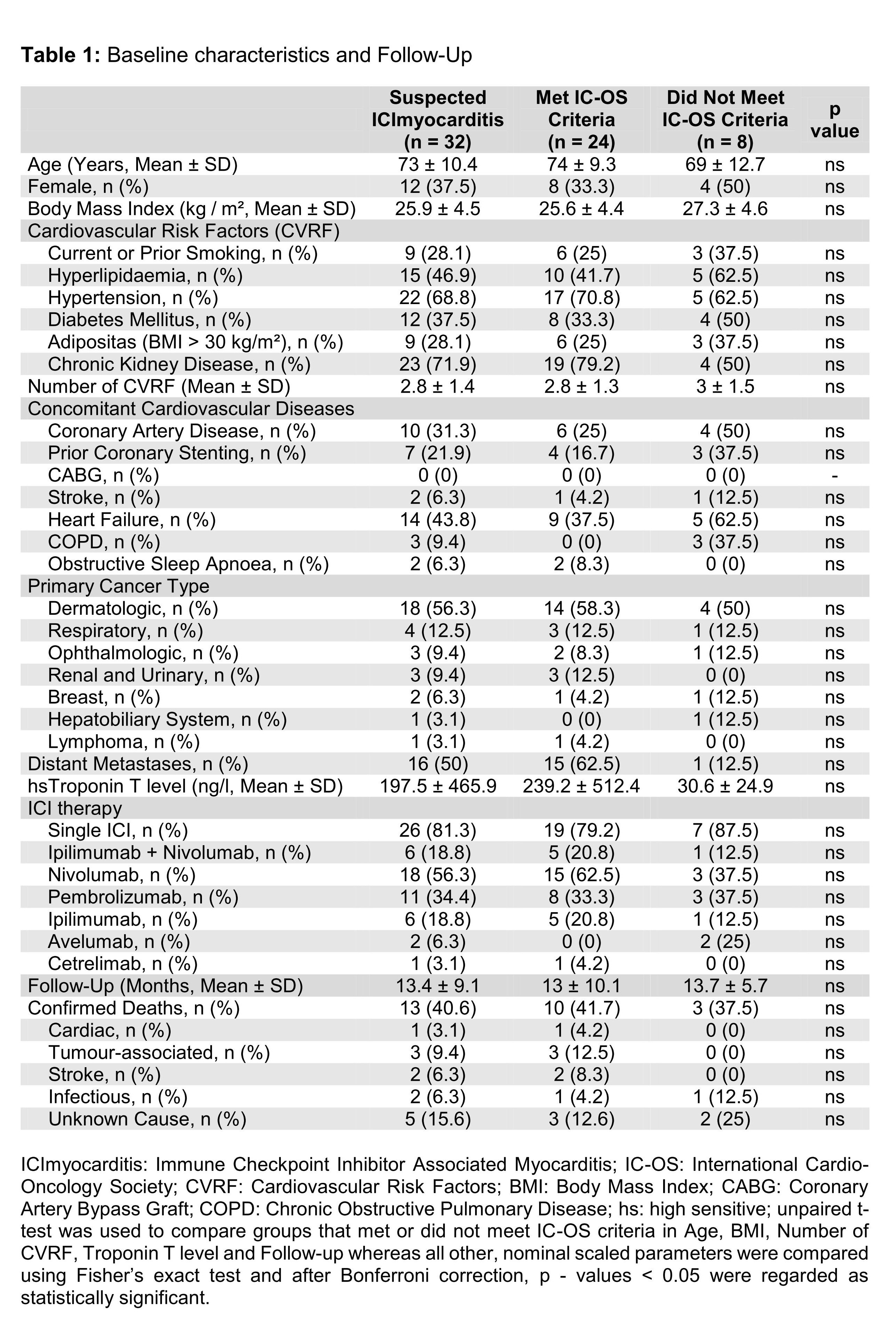
We performed a retrospective analysis of 32 patients’ medical records referred to our cardiology department with suspected ICImyocarditis in 2022 - 2024. Diagnostic workup included Tn in 94%, ECG in 91%, cMRI in 88% and EMB in 41% of cases. 24 patients met IC-OS criteria. Baseline characteristics and follow-up are shown in Table 1. Statistical analysis used Fisher’s exact or unpaired t-test; after Bonferroni correction, p < 0.05 was considered significant. Of 24 confirmed cases, 3 were diagnosed histologically via conclusive EMB and 3 by cMRI meeting the revised Lake Louise criteria. In 18 cases, however, multimodal assessment was necessary to establish diagnosis. When comparing baseline data, those who met IC-OS criteria tended to be older, more often male, had fewer cardiovascular risk factors and comorbidities but a higher rate of distant metastases and higher Tn levels upon admission, without reaching statistical significance. 66.7% of confirmed cases were treated in one oncology centre, where 464 patients were initiated on ICI in 2022 - 2024. In this cohort, ICImyocarditis incidence was 3.4%. Applying the 2018 American Society of Clinical Oncology Clinical Practice Guideline, 18 patients had a mild or moderate ICImyocarditis, 4 were asymptomatic and only 2 presented with severe disease. Of these 2 cases, 1 is the only recorded cardiac death. Mean follow-up was 13.4 ± 9.1 months. We recorded 13 deaths, of which 3 were tumour-associated, 2 infectious, 2 strokes, 1 cardiac and 5 of unknown cause.
Discussion
ICImyocarditis remains a diagnostic challenge. In 75% of confirmed cases, no single test provided diagnostic certainty, emphasizing the need for multimodal assessment and attention to minor criteria. Suspected cases should be referred to specialised cardio-oncology centres. Notably, our case series suggests a higher incidence than previously reported. 91.7% of our patients presented with non-severe ICImyocarditis. Even when including all deaths of unknown cause, the possibly attributable mortality reached only 18.7%. We hypothesize that close clinical monitoring has revealed previously underreported, less severe cases. Early intervention might prevent progression to severe, high-mortality ICImyocarditis. Close interdisciplinary cooperation including repeated cardiologic assessment may further improve outcomes.