AIMS: Diastolic dysfunction is central to heart failure with preserved ejection fraction (HFpEF), yet conventional
echocardiographic measures only approximate left ventricular (LV) filling pressures. Elevated filling pressures also
reflect congestion in heart failure with reduced ejection fraction (HFrEF), influencing symptoms and outcome.
Integrating pressure and volume data enables non-invasive pressure–volume loop (PVL) analysis, allowing direct
assessment of diastolic properties. We examined the prognostic impact of elevated filling pressures compared
with intrinsic diastolic dysfunction in HFrEF and HFpEF.
METHODS: Patients undergoing cardiac catheterization with LV end-diastolic pressure (LVEDP) measurement
between 2018 and 2020 were included. Echocardiography was performed during the same visit. Patients were
classified as HFrEF (LVEF < 50%) or preserved LVEF (≥50%), the latter stratified by the H₂PEFF score into
controls (0–1 points) and suspected HFpEF (≥2 points). Filling pressures were estimated by E/e′. Diastolic
function was quantified by the single-beat diastolic stiffness constant β from PVL analysis and by a simplified
index (E/e′/EDV). The primary endpoint was 5-year all-cause mortality.
RESULTS: Among 496 patients (median age 72 [64–81] years, 37% female), 72 were controls, 176 HFrEF, and
248 suspected HFpEF. LVEDP and E/e′ showed weak correlation (r = 0.17, p < 0.001). Elevated filling pressures
(top E/e′ tertile) occurred in 49% of HFrEF, 30% of HFpEF, and 4% of controls; diastolic dysfunction (top β tertile)
in 40%, 35%, and 8%, respectively. Patients with elevated filling pressures showed reduced survival in HFrEF (p
= 0.010), suspected HFpEF (p < 0.001), and controls (p < 0.001). Diastolic dysfunction by E/e′/EDV predicted
mortality in suspected HFpEF (p = 0.028) but not HFrEF (p = 0.26). In contrast, PVL-derived β was associated
with outcome in both HFrEF (p = 0.017) and suspected HFpEF (p < 0.001).
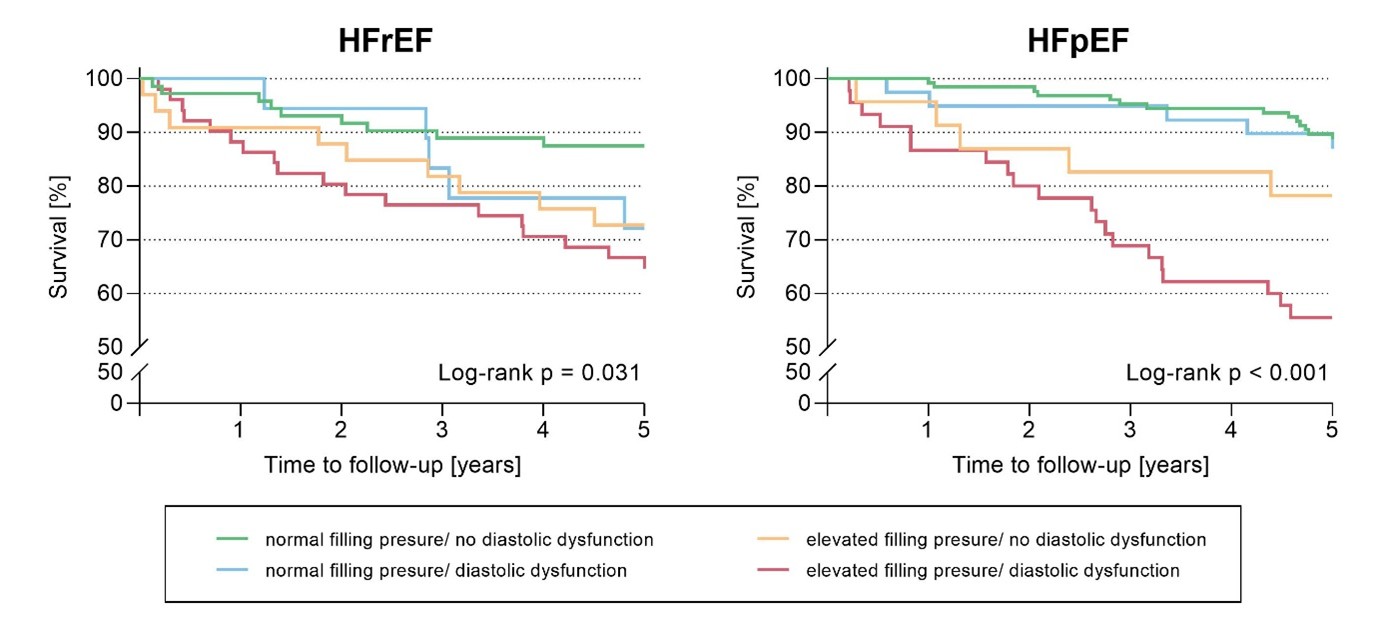
Combining both indices revealed the best prognosis in patients with normal filling pressures and preserved
diastolic function, whereas any abnormality, especially their combination, was linked to poorer survival (Figure 1).
CONCLUSION: This study highlights important limitations of interpreting elevated filling pressures as surrogate
for diastolic dysfunction. Nevertheless, echocardiographic assessment of the E/e’ ratio is an important tool
estimating LV filling pressures among heart failure phenotypes. Adding diastolic dysfunction to the concept allows
for the identification of patients at risk particularly in HFpEF. As non-invasive assessment of diastolic function
remains challenging, non-invasive PVL analysis may overcome these limitations, offering potential for improved
risk stratification and therapeutic decision-making.