Introduction The extent of myocardial injury during pulmonary vein isolation (PVI) using pulsed field ablation (PFA) may influence long-term rhythm outcomes. However, the relationship between biomarker release, ablation geometry and atrial fibrillation (AF) or atrial flutter (AFlu) recurrence remains unclear.
Aim In our previous analysis, we identified an inverse relationship between post-procedural troponin levels and AF/AFlu recurrence. This study aimed to confirm these findings with a larger cohort and longer follow-up and to explore whether high-sensitivity troponin T (hs-cTnT) kinetics relate to ablation map characteristics.
Methods We retrospectively analysed 138 patients undergoing first-time PVI for paroxysmal or persistent AF between 02.2024 and 03.2025, predominantly (134/138) with PFA. In 19 patients, left atrial (LA) high-density(HD) 3D maps were acquired pre- and post-ablation to quantify ablated LA area. Hs-cTnT was measured before ablation and on post-procedural days 1&2; the Δ between baseline and peak values was analysed. Clinical follow-up assessed arrhythmia recurrence.
Results Mean age was 69±11 years; 52 patients (38%) were female and 64% had paroxysmal AF. Mean CHA₂DS₂-VA score was 2.9±1.6. Skin-to-skin time was 59±32min without and 88±43min with HD-mapping. 75 patients were treated with Medtronic™ PulseSelect (PFA-P), 48 with Boston™ Farapulse (PFA-F), 11 with Sphere9™ in PFA-mode (PFA-A) and 4 with radiofrequency ablation with Thermocool® SF. All remapped patients received PFA-P. Mapping catheters were Orion™, HD Grid™ and Octaray™. The ablated area was calculated as a percentage of total LA surface (EnSiteX™) or volume (RHYTHMIA™, CARTO™).
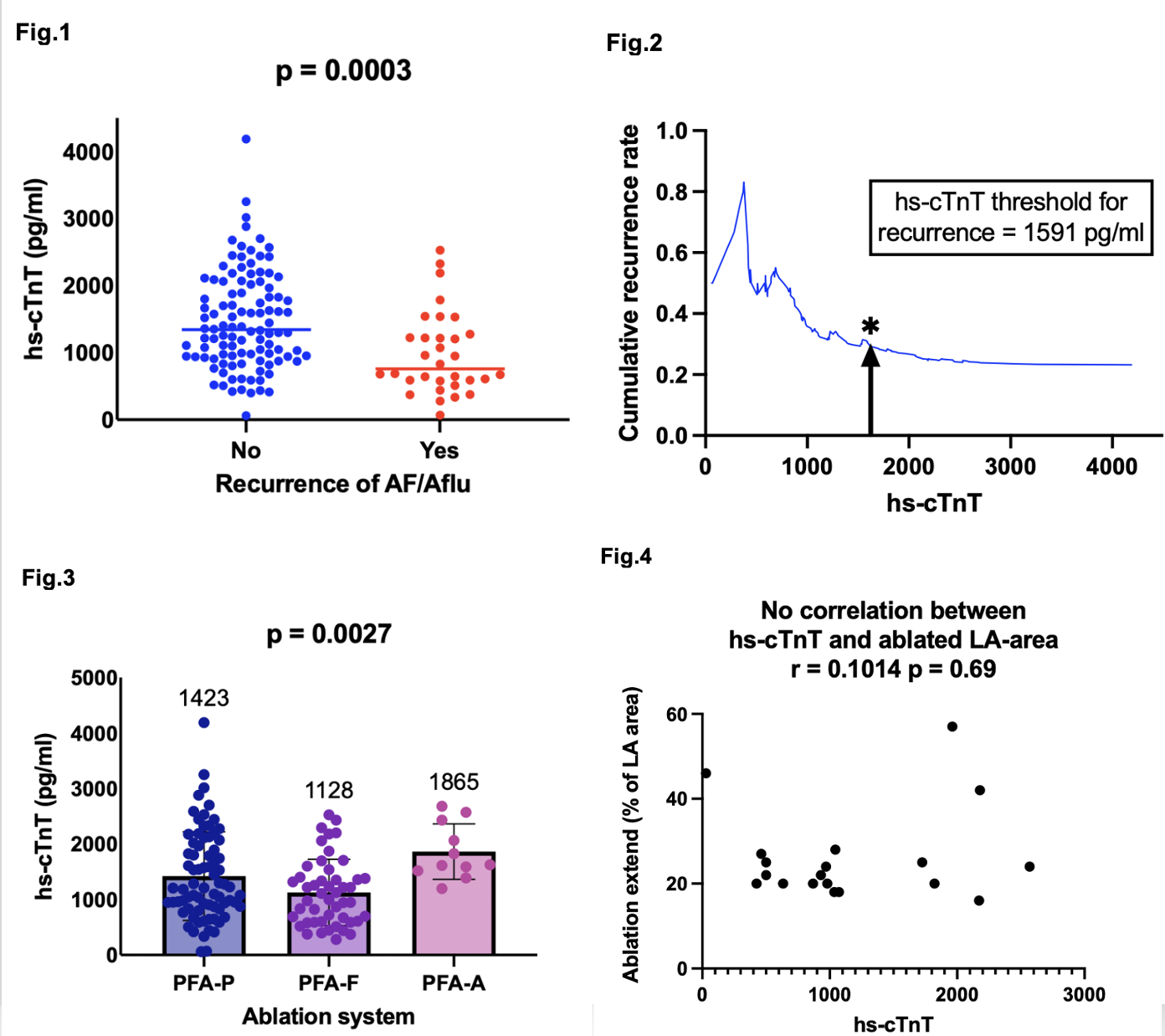
During a median follow-up of 167±84 days, 32 patients (23%) experienced AF/AFlu recurrence. Patients without recurrence had significantly higher hs-cTnT levels than those with recurrence (median 1343 vs 760 pg/ml, p = 0.0003;Fig.1). The calculated recurrence hs-cTnT-cutoff was 1591 pg/ml (Fig.2). Median hs-cTnT release differed significantly among systems (PFA-P 1423, PFA-F 1128, PFA-A 1865 pg/ml; p = 0.0027;Fig.3) but recurrence rates did not between modalities (p = 0.12). No relevant correlation was found between hs-cTnT and ablated area using pearson´s rank correlation (r = 0.10, p = 0.69;Fig.4) or between ablated area and AF/Aflu recurrence (p = 0.25).
Conclusion PFA lesions during PVI are not homogeneously distributed and 3D mapping reflects lesion geometry rather than transmurality. Higher hs-cTnT release after PFA-PVI indicates myocardial cell damage and is associated with improved rhythm outcomes, independent of ablation area. Troponin may therefore serve as a surrogate marker of lesion effectiveness in PFA, whereas geometric extent alone does not predict clinical efficacy. Hs-cTnT measurement could enable immediate post-procedural assessment of ablation success without additional mapping.