Background: Patients with suspected acute coronary syndrome (ACS) are at increased risk of mortality. Periodic repolarization Dynamics (PRD), a marker of sympathetic overactivity, is a strong predictor of mortality after ACS, but it’s application in everyday clinical practice is limited, as it requires 20-minute ECGs. We have recently introduced a novel method of calculating PRD from standard 10-second 12-lead ECG recordings (PRDshort).
Purpose: To assess the long-term mortality risk of patients with suspected ACS using PRDshort.
Methods: Between 1/2014 and 11/2021 we retrospectively identified patients (positive ethics vote 21-1180)who underwent coronary angiography (CA) due to suspected ACS at two tertiary centers in Munich, Germany. Inclusion criterion was availability of raw ECG-data. Exclusion criteria were STEMI and pacemaker stimulation. PRDshort was automatically calculated from ECG raw data and the established cut-off value of ≥/<5.75 deg2 was used. The primary endpoint was 5-year all-cause mortality and was performed using death records. Survival curves were estimated by the Kaplan-Meier method. Predictors of mortality were analyzed using Cox-regression analysis. Multivariable models were adjusted for age, sex and left ventricular ejection fraction (LVEF).
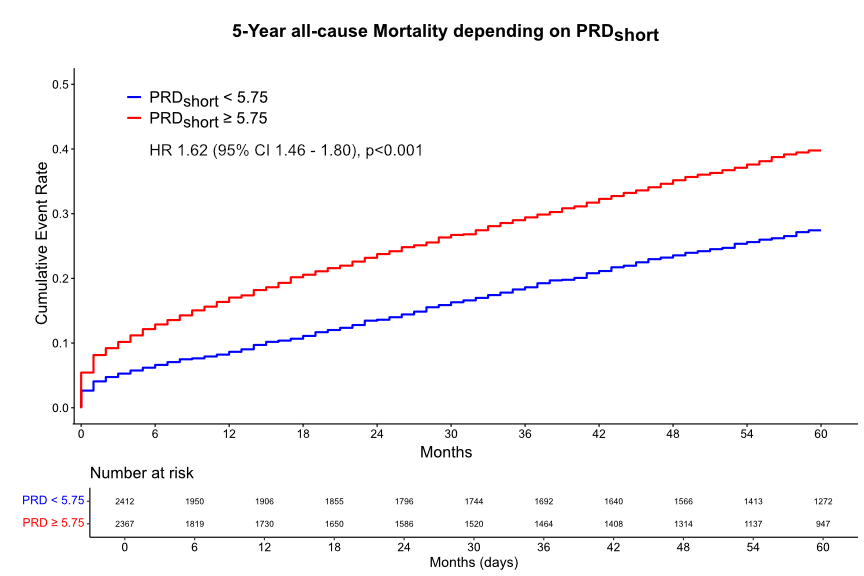
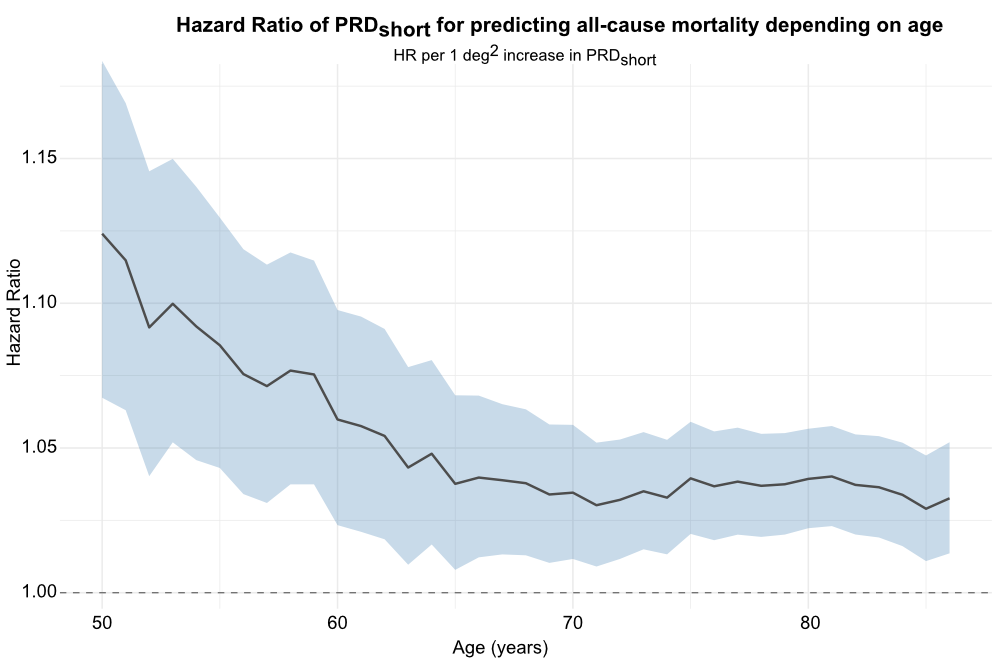
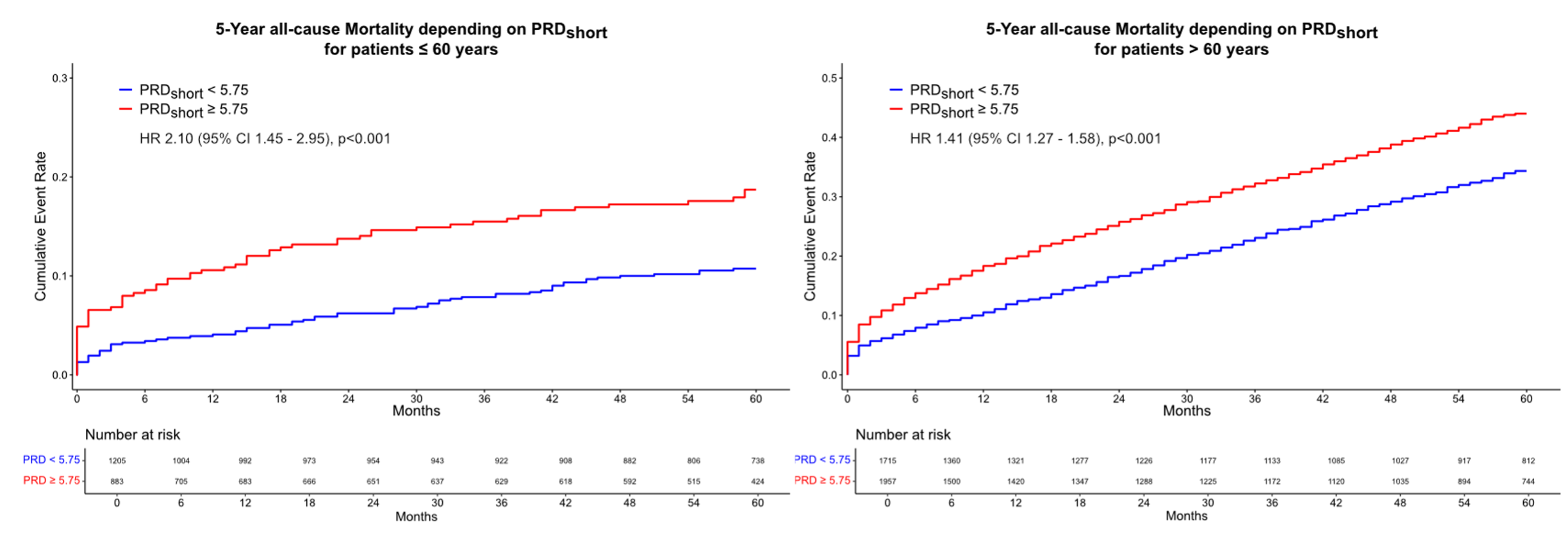
Results: We retrospectively identified 10,266 patients undergoing CA due to suspected ACS. Of these, 4,790 patients (age 70; IQR 62-80 years, 30% females had available ECG raw data and were included in the study. Mean follow-up time was 53 months during which a total of 1,745 patients (36%) died. PRDshort ≥5.75 deg2 was associated with increased 5-year all-cause mortality (HR 1.62, 95%CI 1.46 – 1.80, p<0.001, Fig.1), which remained significant after adjustment for age, sex and LVEF < 40% (HR 1.32, 95% CI 1.18 – 1.47, p<0.001). Analysis of PRDshort depending on age showed that this effect was especially strong in younger patients but stayed significant also in the elderly (Fig.2&3, p-interaction = 0.048). PRDshort ≥5.75 deg2 in patients ≤ 60 years was associated with a 2-fold increase in 5-year mortality (HR 2.10, 95%CI 1.45 – 2.95, p<0.001).
Conclusion: PRDshort is a fully automated autonomic risk tool that can be routinely assessed using standard 10-second 12-lead ECGs. It offers a high predictive value for 5-year all-cause mortality independently from age, sex and reduced LVEF in patients with suspected ACS. PRDshort can be used as a cost-effective and rapid assessment to guide long-term monitoring following ACS.