Background/Introduction: Patients with clinically significant aortic stenosis (AS) referred for transcatheter aortic valve implantation (TAVI) may also have concomitant transthyretin amyloid cardiomyopathy (CA). Different likelihood scores have been proposed to help identify those with dual pathology (AS-CA). Echocardiographic assessment distinguishes different AS flow groups: high-gradient (HG), classical low-flow, low-gradient (cLFLG), paradoxical low-flow, low-gradient (pLFLG) and normal flow, low-gradient (NFLG). Previously, AS-CA was thought to be particularly prevalent in patients with pLFLG AS.
Purpose: To assess differences in likelihood scores for dual pathology (AS-CA) across different aortic stenosis flow groups.
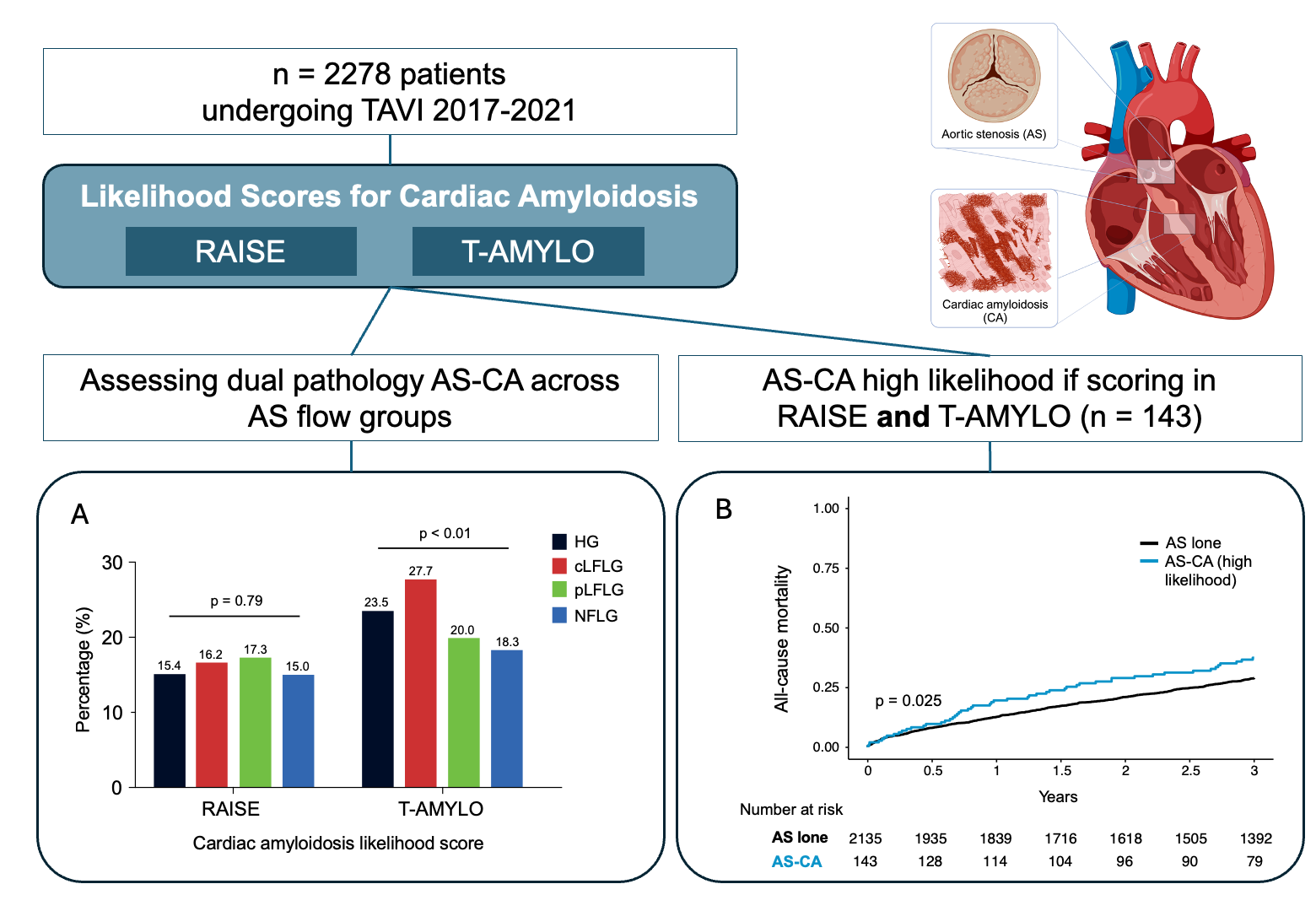
Methods: Three established CA likelihood scores, RAISE (Remodeling, Age, cardiac Injury, Systemic and Electrical abnormalities) score, T-AMYLO (carpal Tunnel syndrome, Age, Male gender, hYpertrophy, LOw QRS voltage) score, and ATTR-CM score were calculated based on chart review for all consecutive patients undergoing TAVI for native severe AS at our centre between 2019 and 2021. Score-specific cut-offs for likely CA were ≥3 points for RAISE, ≥3 for T-AMYLO, and ≥6 for ATTR-CM, respectively. Score results were compared in the context of different AS flow groups. Combined Valve Academic Research Consortium 3 (VARC-3) endpoints and 3-year all-cause mortality following TAVI were analysed stratified by CA likelihood scores.
Results: Among all 1500 patients (57% male, median age 82 [77-85] years), likelihood scores estimated presence of AS-CA in 16.1% (RAISE), 20.4% (T-AMYLO) and 34.7% (ATTR-CM), respectively. According to the RAISE and T-AMYLO scores, CA was most likely among patients with cLFLG AS, whereas the ATTR-CM score suggested a higher likelihood of CA in HG and pLFLG AS (Figure). The likelihood of CA was lowest in NFLG AS. No significant differences in the combined VARC-3 endpoints of technical success or device success were observed concerning the AS-CA likelihood score results. However, mortality differences related to AS-CA were found for the T-AMYLO (p=0.022) and ATTR-CM score (p=0.022), but not the RAISE score (p=0.061). Additionally, no mortality differences were observed across different AS flow groups.
Conclusion: The application of the three CA likelihood scores reveals considerable variability in the estimated likelihood of dual pathology of AS and CA. This may partly be attributable to the different criteria used within the scoring systems, which may not fully capture the high interindividual variability of the multisystemic disease. In contrast to our hypothesis, two out of three scores showed a higher likelihood of CA in patients with classical but not paradoxical LFLG AS. Given the emerging therapeutic approaches in both entities, the coexistence of AS and CA requires further investigations.