Background: Infections are a common complication during post-cardiac arrest syndrome (PCAS) after out-of-hospital cardiac arrest (OHCA). Inflammatory reactions during PCAS make infections hard to diagnose by regular parameters. Studies on the microbial profile and concomitant antibiotic treatment of OHCA patients during PCAS and implications for outcomes are scarce.
Aim: The aim of this study was to evaluate the impact of the microbial profile and antibiotic treatment in the early post arrest period on survival.
Methods: All adult non-traumatic OHCA admitted to a metropolitan University Hospital from 2024-2025 were retrospectively analyzed. Only patients surviving to the intensive care unit were included. All patients with signs of aspiration were treated with antibiotics according to local protcol. All available microbial/viral samples (Blood cultures and serology, Bronchoalveolar Lavage (BAL), urine cultures, swabs) testing for bacterial, viral or fungal pathogens taken < 48 hours after admission were analyzed. Early (< 24 hours) antibiotic treatment was analyzed. The primary endpoint was survival to discharge.
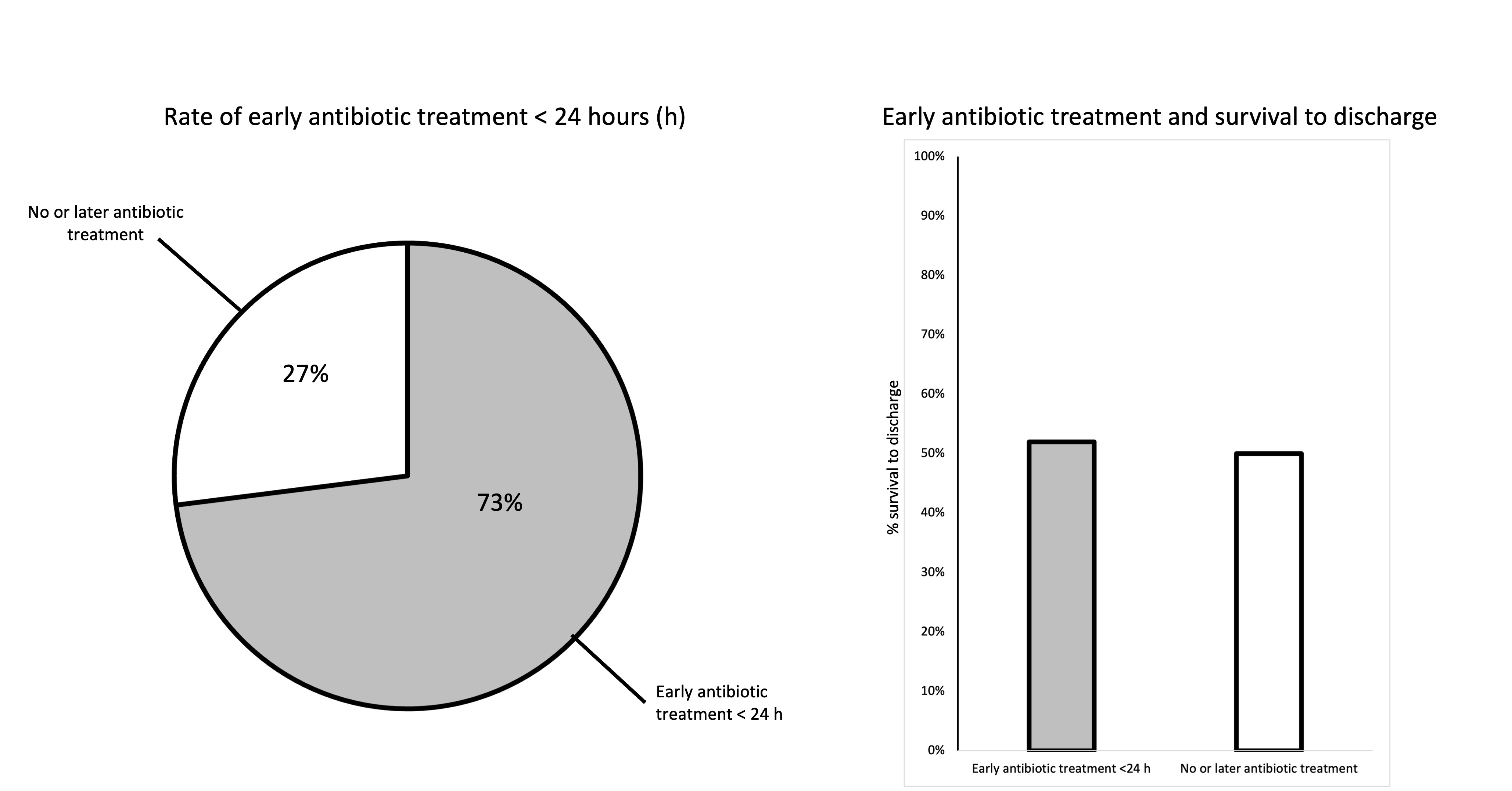
Results: 208 patients were included with an overall median age of 63 years, 26% females, a bystander CPR rate of 59% and an overall survival to discharge of 50%. The most common causes of arrest were primary arrhythmic events (32%) and acute myocardial infarction (26%). 54% had any positive microbial or viral samples with any pathogen. 21% were obligate pathogenic organisms. 31% of blood cultures, 69% of BAL samples, and 17% of urine samples tested positive for any pathogen. Viral pathogens were rare (15 patients). 6% patients had multidrug resistant bacteria. 73% received early antibiotic treatment < 24 hours and mostly ampicillin/sulbactam and piperacillin/tazobactam were given. 22% received single-shot antibiotic treatment. Microbial findings and type of pathogen had no significant impact on survival to discharge. Early antibiotic treatment < 24 hours did not lead to better survival to discharge than late or no antibiotic treatment (52% vs 50%). Excluding patients not surviving until 48 hours after admission showed that patients without detection of any pathogen had significantly better survival to discharge (69% vs 53%, p=0.036, available n=171) while early antibiotic treatment remained without significant impact on survival.
Conclusion: In this study detection of microbial pathogens and early antibiotic treatment during post-cardiac arrest syndrome did not influence survival to discharge. The study includes a highly selected OHCA population in the most critical condition treated at a cardiac arrest center which might mask the influence of the microbial profile and antibiotic treatment on survival. Further studies are warranted to identify factors aiding in decisions making for tailored antibiotic treatment and diagnosing infections in this critical patient group.