Background: Transthyretin amyloidosis (ATTR) has been identified as a growing cause of cardiac disease. Affected patients are usually of an advanced age and have multiple comorbidities, which makes risk stratification challenging and complicates clinical decision-making. The Fried frailty score is a simple, standardised assessment of frailty. The present study evaluated its predictive value for one-year mortality in patients with ATTR amyloidosis.
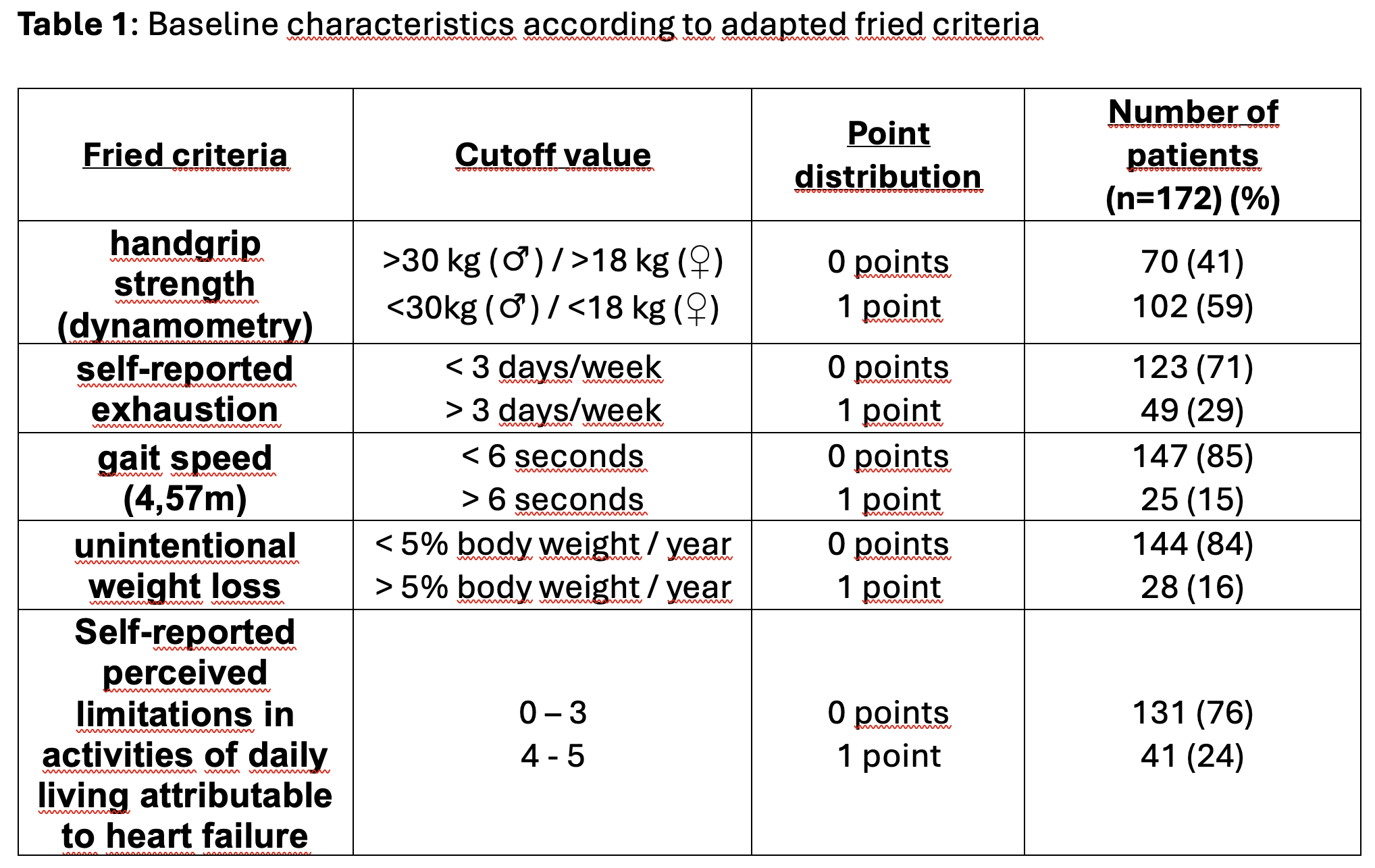
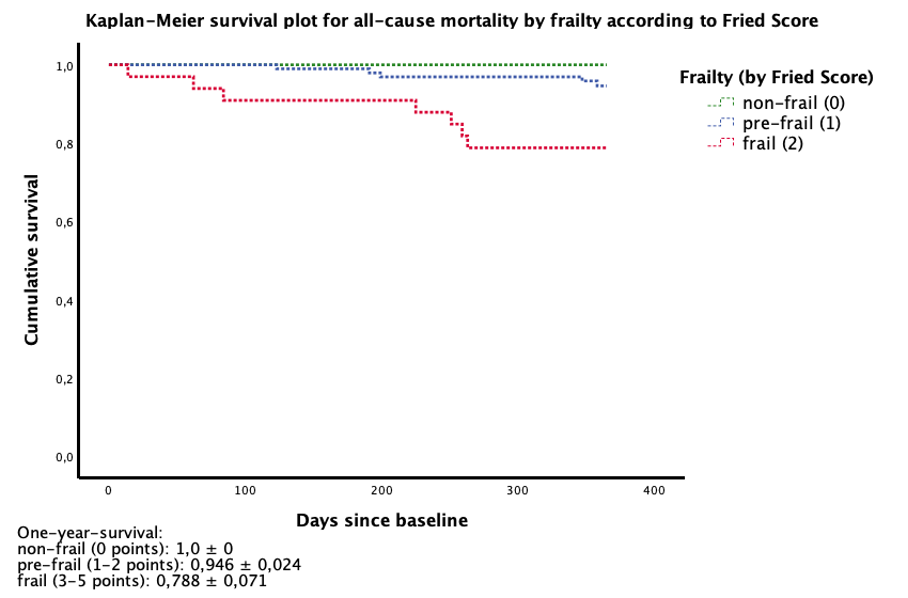
Methods: A single-centre, prospective, longitudinal, observational cohort study was conducted of patients with ATTR who presented at the specialised cardiac amyloidosis outpatient clinic between February 2023 and June 2024. The assessment of frailty was conducted in accordance with the Fried criteria, encompassing five distinct components. The following parameters were considered: handgrip strength, self-reported exhaustion, gait speed, unintentional weight loss and perceived limitations in activities of daily living attributable to heart failure (Table 1). Patients were categorised according to their Fried score as follows: non-frail (0 points), pre-frail (1-2 points), or frail (3-5 points). The primary outcome was defined as all-cause mortality within 365 days from the baseline assessment.
Results: The study comprised a total of 172 patients. Of these, 93 % were male, and the mean age was 80±7 years. According to the Fried score, 42 patients were categorised as non-frail (24.4%), 97 as pre-frail (56.4%), and 33 as frail (19.2%).During the follow-up period, 12 patients (7%) died. The Fried score, when elevated, has been demonstrated to be associated with a higher rate of mortality within a one-year timeframe. The estimated one-year survival probability was 100% (±0%) among non-frail patients, 95% (±2%) among pre-frail patients and 79% (±7%) among frail patients. Each incremental standard deviation of Fried score was associated with an all-cause mortality hazard ratio of 2.39 (95% CI 1.44-9.96; p<0.001).
Conclusion: The Fried criteria have been demonstrated to be a pragmatic and clinically feasible instrument for the assessment of frailty status in ATTR amyloidosis. In the present analysis, elevated Fried scores were found to be strongly and statistically significantly associated with one-year mortality. Consequently, the Fried score has the potential to function as a straightforward prognostic instrument, thereby enhancing risk assessment and informing treatment decisions within the context of routine clinical practice.