Background
Venous vascular closure systems (VCS) are increasingly adopted in interventional electrophysiology to shorten time to ambulation (TTA), alleviate patient discomfort, and minimize vascular complications compared with manual compression or figure-of-eight (F8) suture. Obesity is a recognised risk factor for vascular complications. However, its impact on haemostasis outcomes with and without VCS remains unclear.
Purpose
To assess the impact of obesity on haemostasis following atrial fibrillation (AF) ablation using either a VCS or an F8 suture.
Methods
The STYLE-AF study randomized 125 patients undergoing catheter ablation for AF (≤2 venous access sites) to haemostasis with either a suture-based VCS or an F8 suture, followed by manual compression. Patients were followed for 30 days post-procedure. This subanalysis compared patients with and without obesity (body mass index ≥30 kg/m²) regarding baseline and procedural data, TTA, complications and comfort.
Results
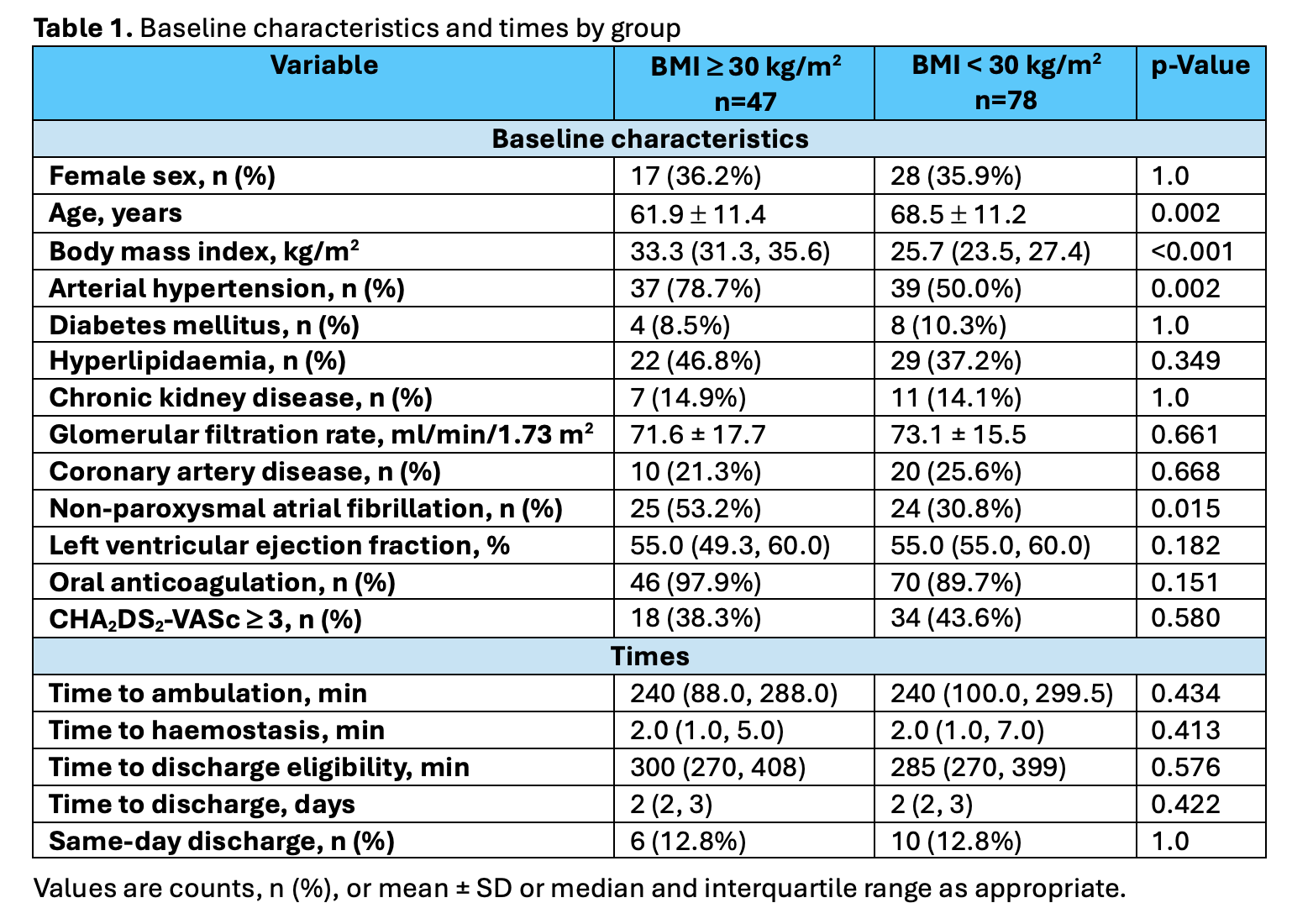
A total of 47 patients (37.6%) presented obesity. Patients with obesity were younger (61.9 ± 11.4 vs. 68.5 ± 11.2 years; p=0.002) and more frequently had arterial hypertension and non-paroxysmal AF.
Cryoenergy was the predominant energy source (85.1% of those with obesity vs. 76.9% of those without), followed by pulsed field ablation (12.8% vs. 17.9%). Two venous access sites were used in most patients (89.4% vs. 82.1%). VCS use was more frequent in patients with obesity (63.8% vs. 42.3%; p=0.027). Procedure and fluoroscopy times were similar, although patients with obesity required higher radiation doses and heparin amounts.
Median TTA did not differ between patients with and without obesity (240 [100–299.5] vs. 240 [88–288] min; p=0.434), irrespective of haemostasis methods.
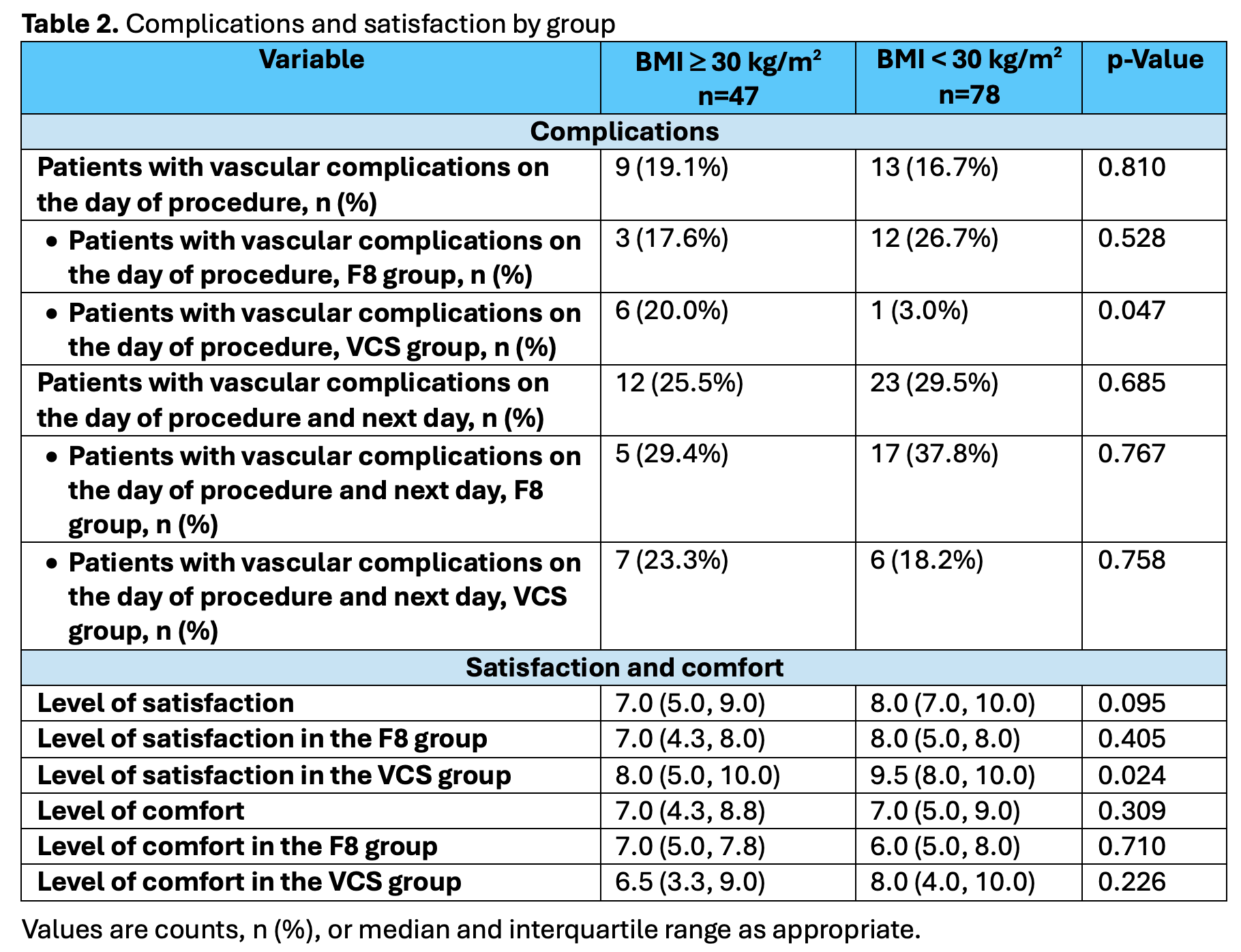
On the day of the procedure, vascular complications occurred in 19.1% vs. 16.7% (p=0.810) of patients with and without obesity. Vascular complications on the day of procedure and the following day occurred in 29.4% vs. 37.8% (p=0.767) of patients with and without obesity treated with F8, and in 23.3% vs. 18.2% (p=0.758) of those treated with VCS. VCS use showed a trend toward fewer vascular complications in patients without obesity (OR 0.366, 95% CI 0.125–1.067; p=0.066) but not in those with obesity (OR 0.730, 95% CI 0.191–2.799; p=0.647). No major vascular complications occurred.
There was a trend toward lower satisfaction regarding the bedrest time in patients with obesity. In patients treated with VCS, satisfaction was significantly lower in those with obesity compared with those without.
Conclusions
TTA was comparable between patients with and without obesity. The relative benefit of VCS in reducing vascular complications appeared less pronounced among patients with obesity. In patients without obesity, the incidence of vascular complications on the day of procedure and the following day was more than twice as high with the F8 compared with VCS. Satisfaction among VCS recipients was lower in patients with obesity.