Introduction: The seasonal influence on acute coronary syndromes is well established with higher incidence and worse outcomes in winter. Data on impact of seasonal changes on the presentation and diagnosis of non-acute coronary artery disease (CAD) is lacking. Aim of this study was to evaluate the influence of seasons on the diagnosis of CAD by coronary CT-angiography (CCTA).
Methods: Data from a high-throughput cardiac CT practice was retrospectively analyzed (2020 –2025). Following parameters were compared for each season: CAD defined as presence of atherosclerotic plaques in CCTA. Presence of obstructive CAD defined as a stenosis ≥ 50 % in CCTA. Initiation of new medical therapy and initiation of invasive coronary angiography (ICA) based on the CCTA-findings. Seasons were defined metrologically (Spring: March – May, Summer: June – August, Autumn: September – November, Winter: December – February).
Results: 11785 patients received CT-scans in the study period and 10023 CCTA were included. Excluded were patients with known CAD, calcium-score only CT`s, other CT-protocols, non-diagnostic CT. CAD was diagnosed in 61.5% and obstructive CAD in 33.4% of patients. No significant seasonal differences were observed in CAD diagnosis. Obstructive CAD tended to be more likely diagnosed in spring (35.1%) and summer (34.1%) compared to autumn (31.4%, winter 32.6%) and patients were 18% (OR 1.181; CI 95% 1.048 – 1.330; p=0.006) more likely to be diagnosed with obstructive CAD during spring and 13% (OR 1.130 CI 95% 1.001 – 1.276; p=0.048) during summer compared to autumn. While new medical therapy initiation remained stable throughout the seasons, significant seasonal differences were observed in the initiation of ICA (Spring to winter: 10.6%, 9.7%, 8.5%, 7.9%, p=0.004) and initiation of ICA was 38% more likely during spring (OR 1.382 CI 95% 1.140-1.674, p<0.001, Reference: winter).
Conclusion: In this large retrospective real-world population, there were significant trends in seasonal differences in first-time diagnosis of obstructive CAD. The significantly increased initiation of ICA might indicate more hemodynamically relevant stenosis in CCTA or severe clinical presentation during spring and summer. Since seasons might affect routine clinical practice, further studies should evaluate these possible seasonal trends.
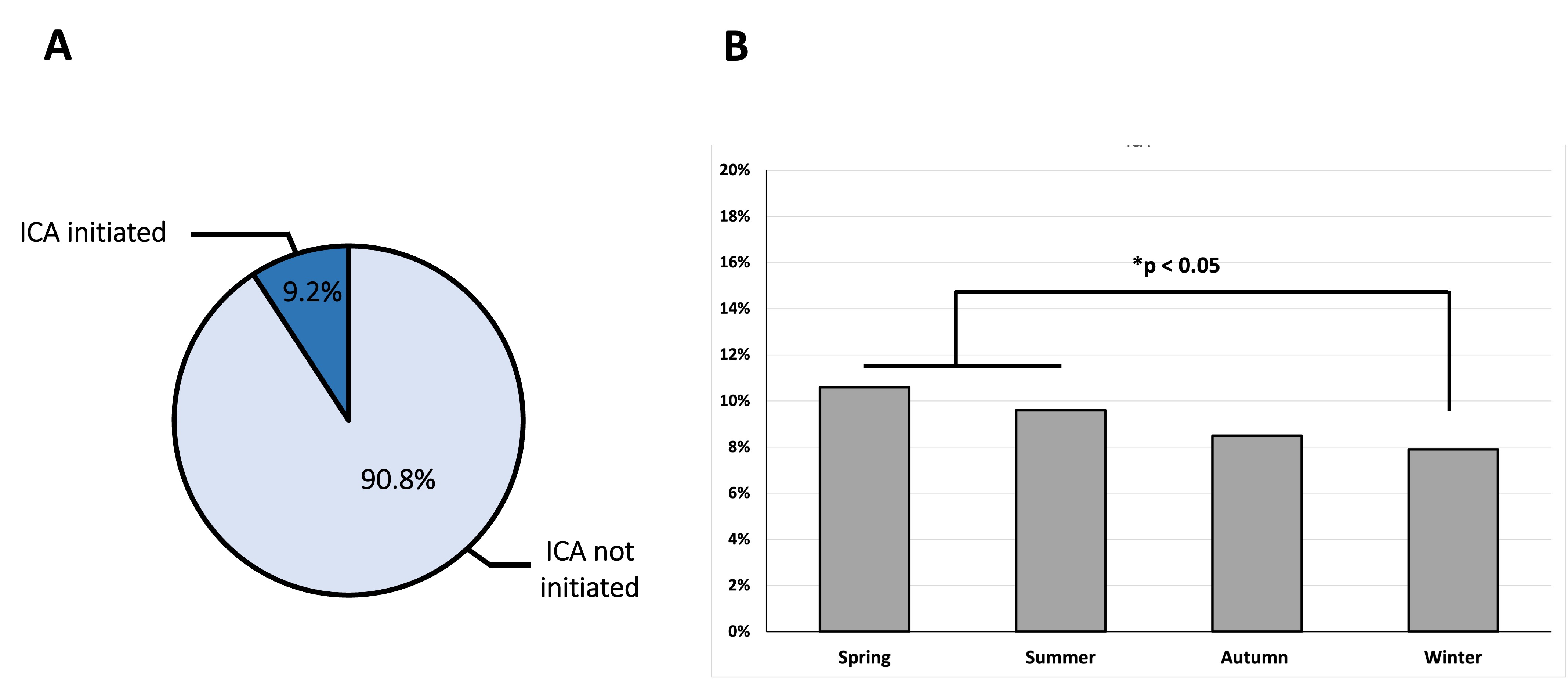
Figure: Initiation of invasive coronary angiography (ICA) based upon coronary CT-angiography findings. A: In the overall study population. B: Stratified by seasons. *p < 0.05 significant in logistic regression.



