Percutaneous coronary intervention (PCI) of the left circumflex artery (LCX) carries a particular risk of left atrial injury due to close anatomical proximity. We report a rare and instructive case highlighting early imaging-based recognition and interdisciplinary management of an iatrogenic left atrial dissection following PCI.
A 40-year-old male presented with acute chest pain and inferolateral ST-segment depression. Urgent coronary angiography revealed distal LCX occlusion consistent with non-ST-elevation myocardial infarction. During PCI, an anatomically adjacent left atrial branch was inadvertently wired and stented, resulting in vessel perforation. To exclude the perforation, the true LCX was subsequently wired and sealed with a covered stent. Despite initial angiographic success, the patient rapidly developed cardiogenic shock with severe pulmonary edema.
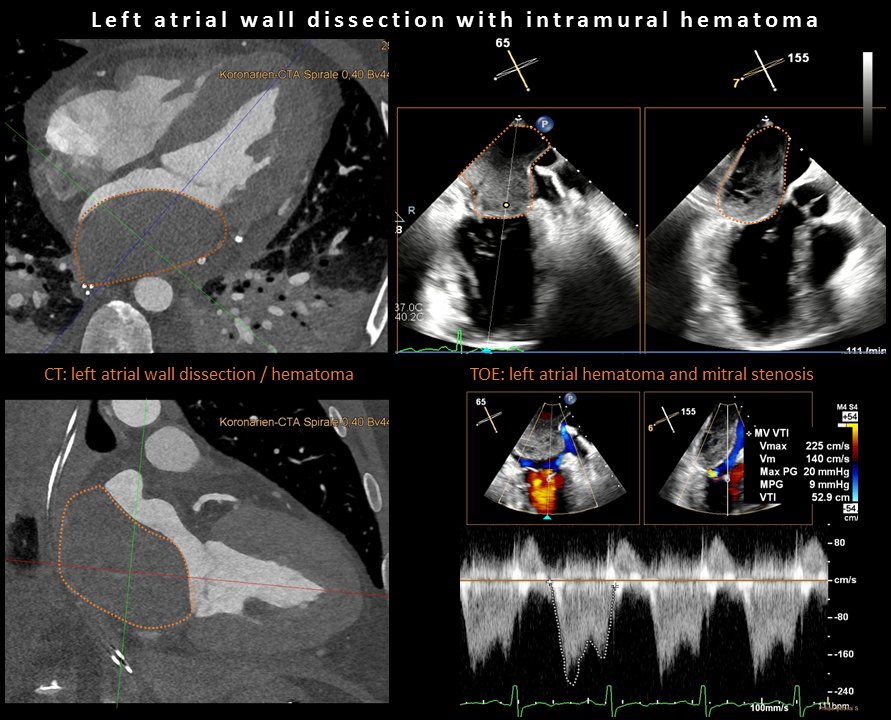
Transesophageal echocardiography (TOE) demonstrated a large left atrial mass (45 × 55 mm) compressing the mitral inflow tract, causing functional severe mitral stenosis (mean gradient 9-10 mmHg; file 1). Cardiac computed tomography (CT) confirmed a left atrial wall dissection with intramural hematoma extending to the posterior mitral annulus without active leakage (file 1). The patient underwent urgent surgical evacuation via median sternotomy with direct left atrial access and endoluminal incision of the dissection membrane. Postoperatively, due to persistent pulmonary edema, short-term veno-venous extracorporal membrane oxygenation (ECMO) support was initiated for transfer to intensive care and could be successfully weaned within 24 hours.
The postoperative course was favorable with complete recovery. At three-month follow-up, cardiac magnetic resonance imaging (MRI) showed preserved left ventricular ejection fraction (58%) despite a small inferolateral scar and full resolution of the atrial hematoma. Follow-up coronary angiography with optical coherence tomography (OCT) confirmed patent LCX flow but relevant stent malapposition, which was successfully corrected by targeted postdilatation, achieving optimal apposition and TIMI III flow.
This case demonstrates an exceptional PCI complication with inadvertent left atrial stenting and subsequent atrial dissection. Prompt multimodal imaging, surgical evacuation, and optimized postprocedural management were decisive for the favorable outcome. Awareness of this mechanism and close collaboration between interventional cardiology, imaging, and cardiac surgery are crucial for successful complication management.