BackgroundCatheter ablation is the most effective atrial fibrillation (AF) therapy to date, but success rates are still not satisfactory, particularly in persistent AF, where pulmonary vein isolation (PVI) alone may not be sufficient. One likely reason is our limited understanding of individual AF mechanisms. This in turn is in part due to the absence of suitable mapping systems that allow for global beat-to-beat mapping of AF with sufficient spatial resolution.
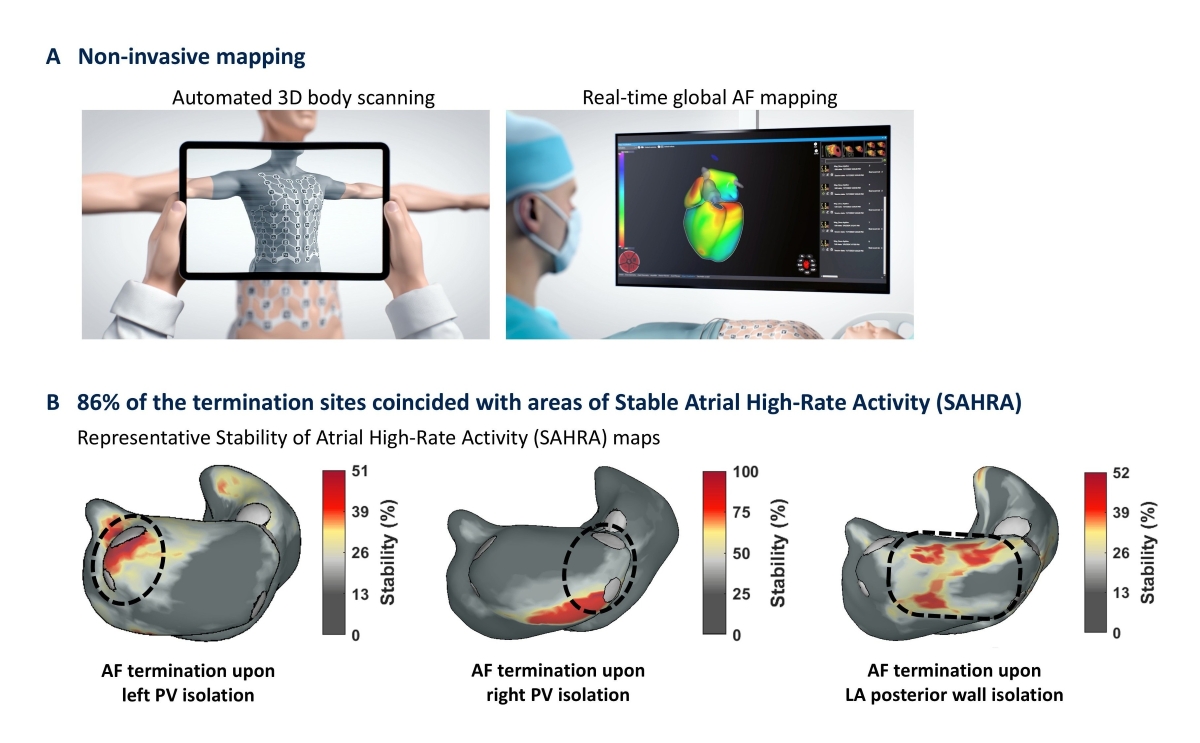
Here we use a novel non-invasive mapping system which enables global beat-to-beat mapping and thus, the assessment of individual spatio-temporal AF dynamics. Using this non-invasive global mapping system, we developed a novel mapping approach to target AF-perpetuating drivers based on the temporal Stability of local Atrial High-Rate Activity (SAHRA). It was tested, to what extent areas of stable high-rate activity matched with termination sites during empirical AF ablation.
Methods and ResultsIn this European multicenter study, a total of 185 consecutive AF-ablation patients that presented in AF were prospectively included and underwent peri- and intraprocedural non-invasive global mapping. In all patients, pulmonary vein (PV) isolation was performed. Additional empirical ablation targets like the left atrial (LA) posterior wall, LA anterior wall, LA appendage or right atrial targets were at the operators’ discretion.
In 42 of the 185 patients (22.7%), isolation of either the left PV antrum, the right PV antrum, the posterior or anterior LA wall or the LAA resulted in AF termination – either conversion to sinus rhythm (20 patients) or transition to an organized flutter (22 patients). In 36 patients (85.7%), the AF termination site coincided with an area of stable atrial high-rate activity according to non-invasive SAHRA mapping and could thus have been defined as ablation target a priori. Three representative cases are shown in Figure 1B.
Overall, SAHRA mapping predicted AF termination sites with high accuracy – the sensitivity (86%), specificity (85%) and particularly the negative predictive value (98%) were high, whereas the positive predictive value was somewhat lower (43%).
Those areas of stable high-rate activity that conincided with AF termination sites displayed a mean cycle length of 149 ms and a spatiotemporal stability over a mean of 60.8 % of the recording period according to SAHRA mapping.
ConclusionStability of Atrial High-Rate Activity (SAHRA) mapping provides a novel, non-invasive method to identify atrial sites that are critical for the perpetuation of AF and thus constitute promising ablation targets. The strong agreement between regions with stable high-rate activity and AF termination sites suggests that SAHRA mapping could become a valuable tool to guide AF ablation and pave the way towards more effective personalized therapies.