BACKGROUND
Patients with classical low-flow, low-gradient (LF-LG) aortic stenosis (AS) and reduced left ventricular ejection fraction (LVEF) undergoing transcatheter aortic valve implantation (TAVI) experience adverse outcomes. Contractile flow reserve (FR), assessed by low-dose dobutamine stress echocardiography, was historically used to identify patients likely to benefit from valve intervention. However, current guidelines remain ambiguous regarding the clinical relevance of FR, and its prognostic value in contemporary TAVI-treated patients remains uncertain.
OBJECTIVEThe study aimed to evaluate the prognostic impact of FR on clinical outcomes in patients with classical LF-LG AS undergoing TAVI, and to contextualize these outcomes relative to a reference cohort with normal-flow, normal-gradient (NF-NG) AS.
METHODS
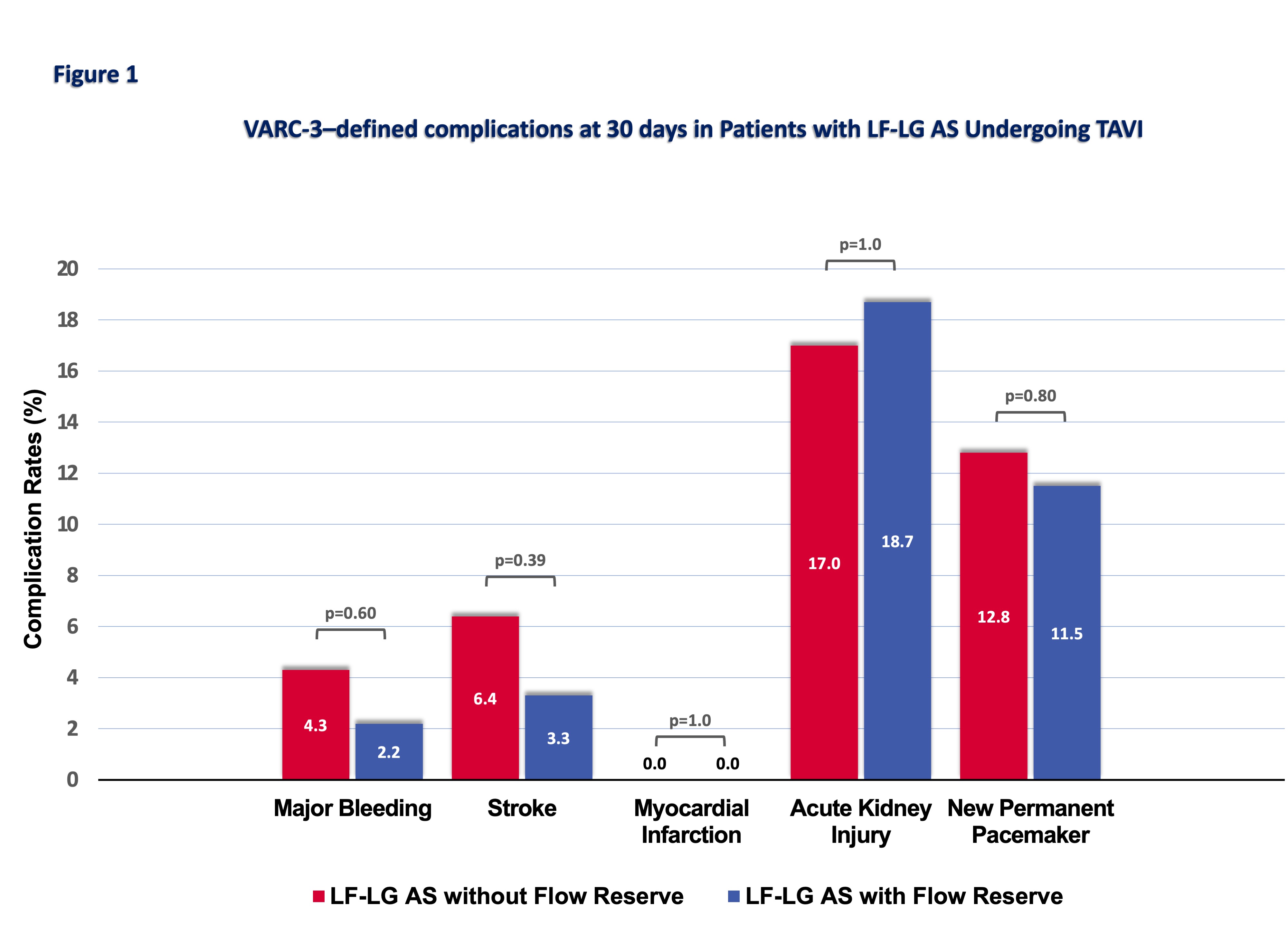
The study cohort included 2,887 consecutive patients undergoing TAVI between 2010 and 2023. Of these, 231 patients (8%) met the criteria for LF-LG AS with reduced LVEF, and among them, 47 patients (20%) lacked FR based on pre-procedural echocardiographic assessment. The primary endpoint was all-cause mortality following TAVI; secondary endpoints included VARC-3–defined complications at 30 days.
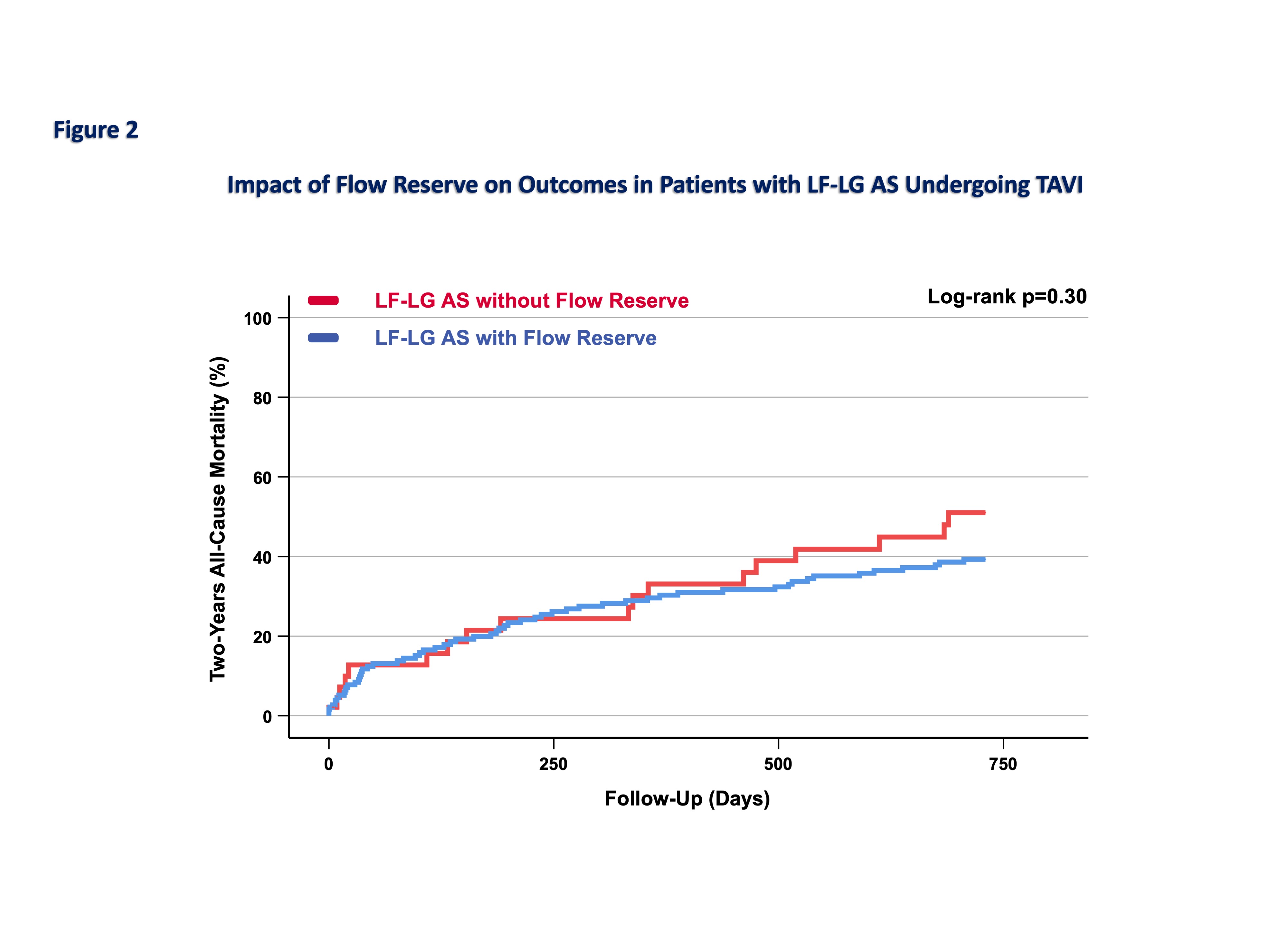
RESULTSThe mean age of the cohort was 80.9±6.4 years, and 46% were female. Compared with patients with NF-NG AS, those with LF-LG AS had more advanced comorbidities, reflected by a higher EuroSCORE II (8.42% [5.0-13.7] vs 3.6% [2.2-6.1], p<0.01) and lower LVEF (35±9% vs 56±11%, p<0.01). Within the LF-LG subgroup, baseline characteristics were comparable between patients with and without FR (p>0.05). Periprocedural complications, including major bleeding, stroke or acute kidney injury, were comparable between LF-LG AS patients with and without FR (Figure 1). Overall, one-year all-cause mortality was significantly higher in patients with LF-LG AS compared with those with NF-NG AS (24.7% vs. 10.3%, p<0.01). Among the LF-LG AS group, patients with and without FR showed comparable 30-day mortality rates (7.6% vs. 10.6%, p=0.55). Similarly, one-year all-cause mortality did not differ significantly between patients with and without FR (25.5% vs. 24.5%, p = 0.85). This finding persisted over two years, as shown in
Figure 2.
CONCLUSION In patients with classical LF-LG AS treated with TAVI, mortality remains substantially higher than in those with NF-NG AS. However, the presence or absence of FR does not significantly influence short- or long-term survival. These real-world findings confirm that patients with LF-LG AS and absent FR represent a clinically relevant and accessible population, and that TAVI is technically feasible and acceptably safe in this high-risk subgroup.