Background: Patients with intermediate (2-3) GLIDE scores for T-TEER represent a clinical grey zone for treating severe tricuspid regurgitation (TR). We sought predictors of T-TEER failure in this subgroup and assessed TTVR performance.
Methods: We analyzed T-TEER failure predictors in the original GLIDE 2-3 cohort and assessed outcomes in a multicenter TTVR registry (n=161). Endpoints were procedural success (discharge TR ≤ moderate) and 30-day outcomes (NYHA, KCCQ-12). KCCQ data was available for 69% of patients.
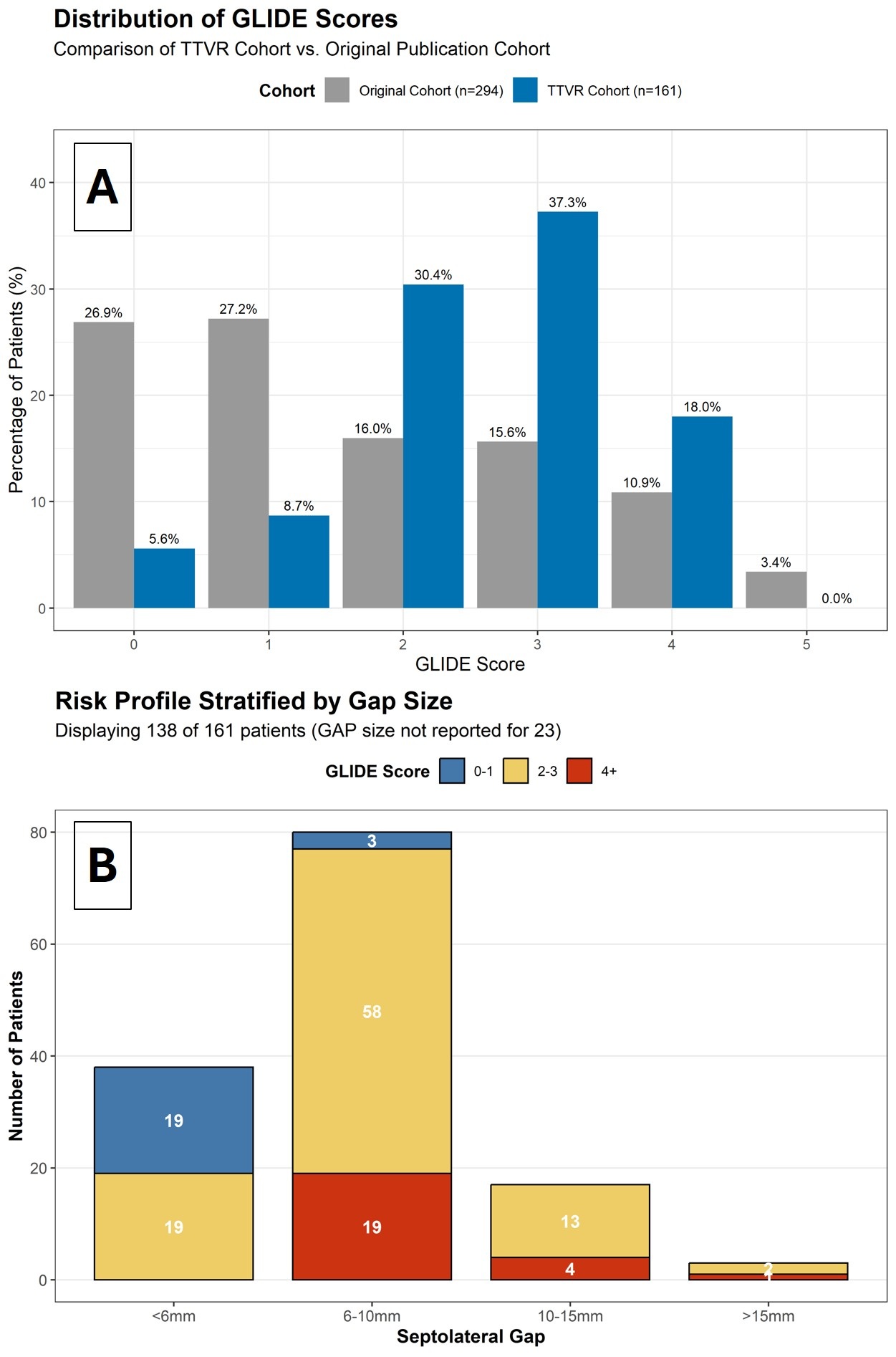
Results: The comparison of distribution of T-TEER and TTVR GLIDE Scores are shown in (Figure A) and demonstrates a shift to higher scores in the TTVR cohort. In the original T-TEER cohort, gap size > 6mm was present in 16.1%. Among patients in the GLIDE 2-3 group with a coaptation gap >6mm, the procedural failure rate was 66%. The TTVR cohort had a high prevalence of gaps > 6mm (72.7%; Figure B). Nevertheless, procedural success was 98.1%. There was a significant 30-day QOL improvement: NYHA from 3 (CI: 3-3) to 2 (CI: 1-2), (p<0.001), and KCCQ from 50.2 to 71.9 (p<0.001). Baseline characteristics and GLIDE score distribution did not differ significantly between patients with and without KCCQ data.
Conclusion: In this registry, TTVR demonstrated a right-shifted GLIDE scores compared to those treated with T-TEER. Procedural success is less likely with T-TEER in intermediate GLIDE score patients with a large coaptation gaps. If clinical risk is acceptable, TTVR may be preferable treatment choice to achieve procedural success with intermediate GLIDE scores and large septolateral gaps.