Background:
Ablation of premature ventricular contractions (PVCs) originating from the Purkinje network, particularly those with multiple exit sites and morphologies, presents a complex clinical challenge. In refractory cases where conventional ablation fails, proximal conduction system ablation may offer a viable alternative.
Objective:
This study evaluated the safety and efficacy of proximal conduction system ablation in patients with multi-exit Purkinje PVCs displaying diverse morphologies.
Methods:
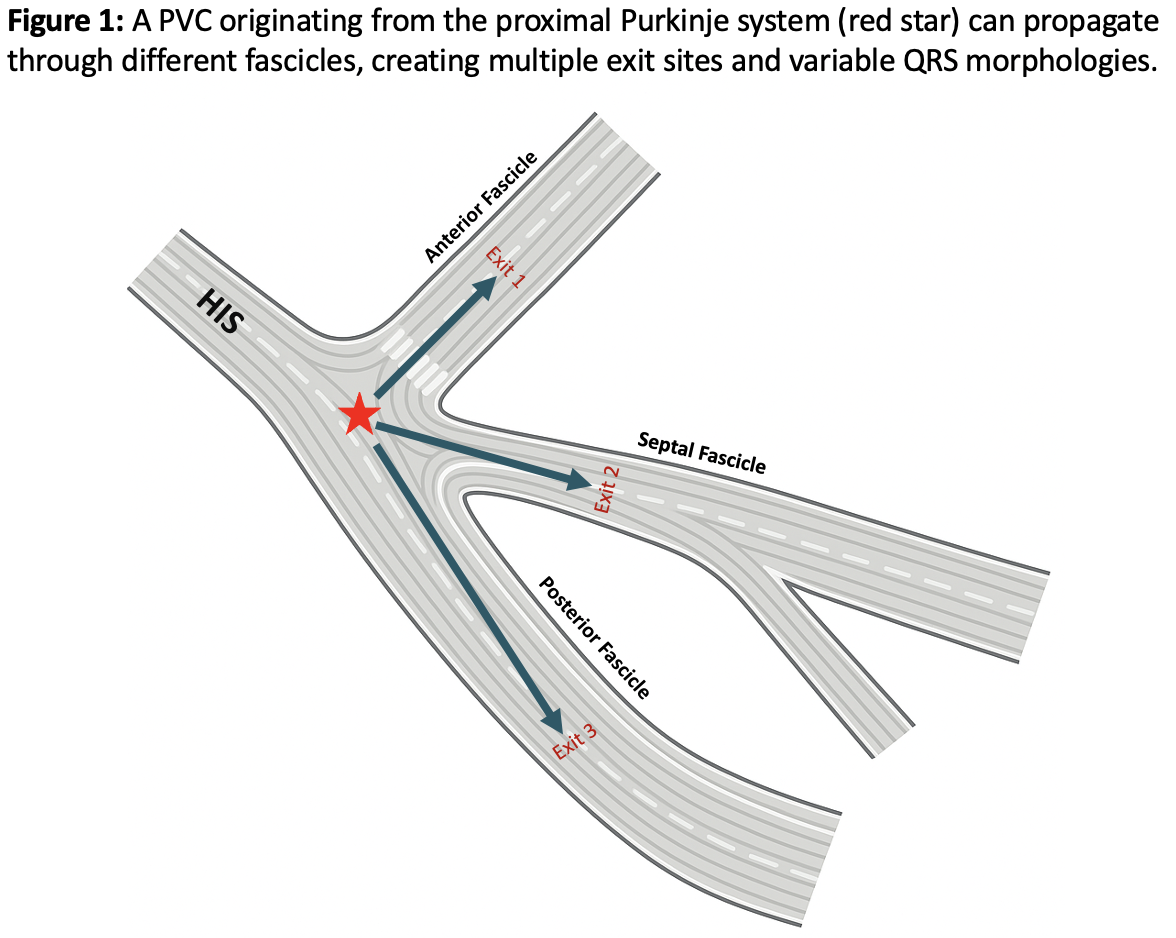
This retrospective cohort included 19 consecutive patients with drug-refractory, symptomatic Purkinje PVCs who underwent proximal conduction system ablation. During ablation, multiple exit sites and morphologies were observed, indicating complex activation within the Purkinje network (Figure 1). Detailed mapping of PVCs was performed to identify the earliest activation and optimal ablation targets within the proximal conduction system.
Results:
Among 19 patients, successful ablation at the proximal Purkinje network was achieved in 17 (89%), while 2 procedures were unsuccessful. Fourteen patients (74%) had PVCs that triggered ventricular fibrillation. The earliest activation arose from the posterior or septal fascicle in 15 patients and the anterior fascicle in 4. All showed a post-ablation shift in the earliest excitation site. Conduction disturbances occurred in five patients: two with complete atrioventricular block, two with posterior fascicular block, and one with anterior fascicular block. During a median follow-up of 21 months (IQR 14.5–47), two patients experienced PVC recurrence requiring repeat ablation, but no ventricular fibrillation recurred.
Conclusion:
Proximal conduction system ablation can be an effective and safe strategy for patients with multi-exit Purkinje PVCs. Larger studies are needed to validate its long-term safety and efficacy.