Importance: CHIP has been associated with several CV diseases and incident AF. However, its relationship with CV outcomes in individuals with preexisting AF is not yet well understood.
Objective: To examine associations of CHIP mutations with MACE, individual CV outcome and AF progression in an AF cohort.
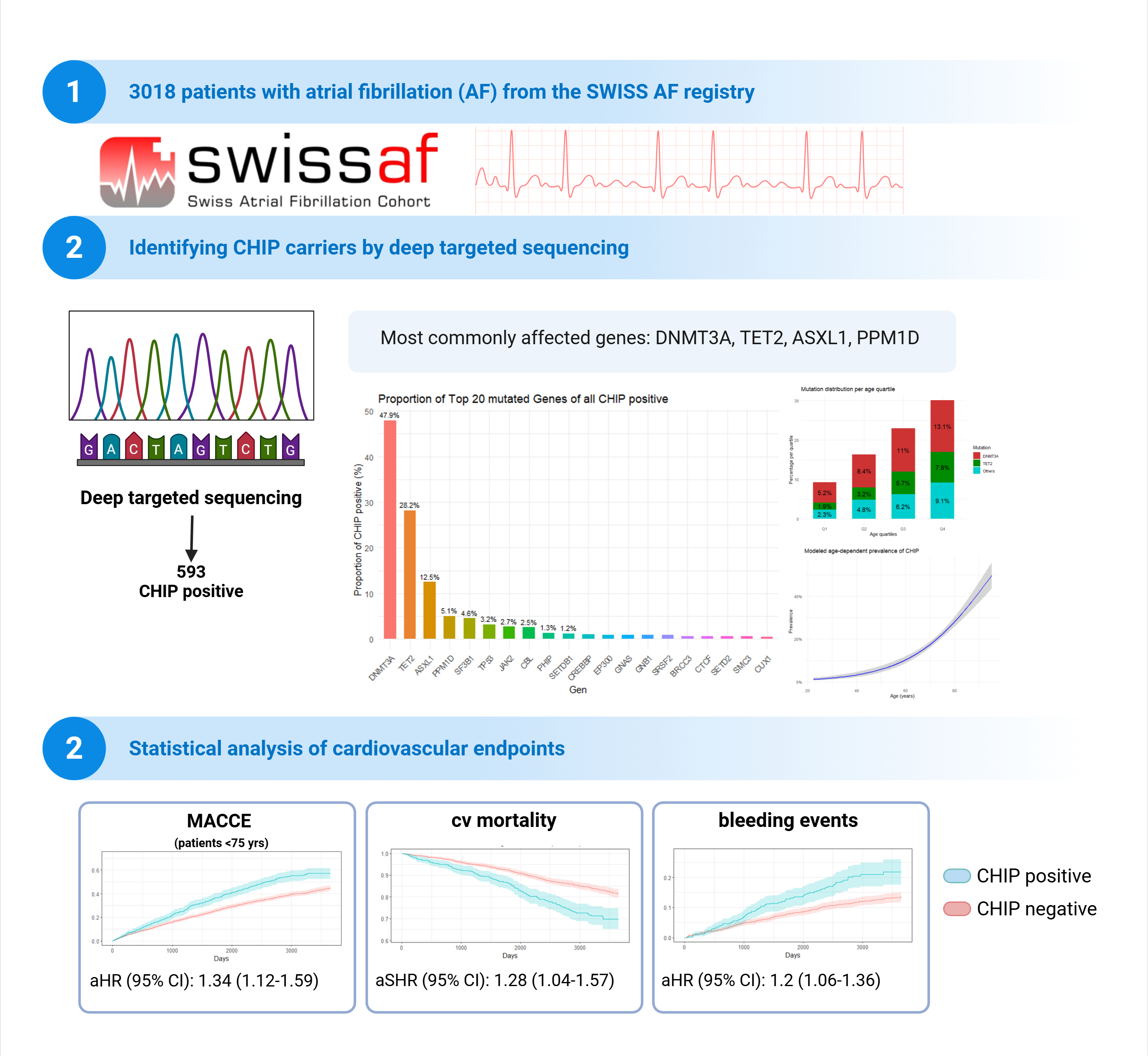
Design, Setting, and Participants: Multicenter cohort study of AF patients from the Swiss-AF study who underwent targeted sequencing for CHIP-related mutations, and standardized clinical assessment between June 1, 2010, and June 13, 2024.
Exposure: Deep-targeted sequencing was performed at baseline. Three CHIP carrier patterns were compared: any CHIP carrier, DNMT3A mutation carriers, and non-DNMT3A mutation carriers (CHIP mutations other than DNMT3A).
Main Outcomes and Measures: Composite and individual cardiovascular outcomes were assessed during the up to 14 years of follow up (Median follow up of 7.5 years). Associations between CHIP and outcomes were assessed using multivariable adjusted logistic and linear regression models and competing risk models. Exclusion criteria included inability to give informed consent, a history of malignancies and secondary forms of AF attributable to reversible causes, such as infection or perioperative AF.
Results: The study included 3,018 AF patients, mean age 70.6 years (SD ± 10.2), 28.2% female participants. CHIP mutations were detected in 593 patients (19.7%), predominantly affecting epigenetic modifier genes DNMT3A (284 patients, 47.9%) and TET2 (167 patients, 28.2%).
CHIP-positive patients demonstrated distinct baseline characteristics, including advanced age, reduced BMI, and higher rates of diabetes, coronary artery disease, and renal impairment. Heart failure history and permanent AF were more prevalent in the CHIP-positive cohort. These patients less frequently underwent rhythm control interventions, receiving fewer pulmonary vein isolations and reduced Type Ic antiarrhythmic prescriptions. Laboratory findings revealed elevated inflammatory markers (hsCRP), and CHIP carriers more commonly required diuretic therapy.
Multivariable-adjusted longitudinal analysis revealed that CHIP carriers under 75 years experienced significantly elevated risk of the composite MACCE endpoint (encompassing mortality, cerebrovascular events, heart failure events, and major hemorrhage), along with increased individual risks of heart failure hospitalization and both major and minor bleeding complications. Notably, CHIP status did not significantly influence AF progression patterns or new-onset heart failure during the observation period.
Conclusions and Relevance: In middle-aged AF populations, CHIP independently confers increased susceptibility to major adverse cardiovascular events and hemorrhagic complications.
Key Words: Atrial fibrillation, clonal hematopoiesis, mortality, heart failure, AF progression, bleeding events
References:
Jaiswal S et al., N Engl J Med. Jul 13 2017;377(2):111-121. doi:10.1056/NEJMoa1701719
Díez-Díez M et al., Nat Med. Oct 2024;30(10):2857-2866. doi:10.1038/s41591-024-03213-1
doi:10.1001/jamacardio.2024.0459