Background:
Blunt chest trauma is frequently accompanied by conduction abnormalities and arrhythmias, reported in up to 20% of cases and independently associated with adverse outcomes. The classic term “contusio cordis” lacks consistent diagnostic criteria. This study introduces the concept of traumatic cardiomyopathy (TCM) and aims to identify echocardiographic and biomarker-based predictors of severe arrhythmic events (SAE) and mortality.
Methods:
In this prospective single-center study 81 polytrauma patients (Injury Severity Score ≥16) were enrolled. High-sensitivity cardiac troponin (hscTn) and NT-proBNP were measured at admission, 24 h, 48 h, day 5, and day 10 after polytrauma. Transthoracic echocardiography (TTE) was performed within 24 h and repeated after 48 h. ECGs were analyzed retrospectively.
Results:
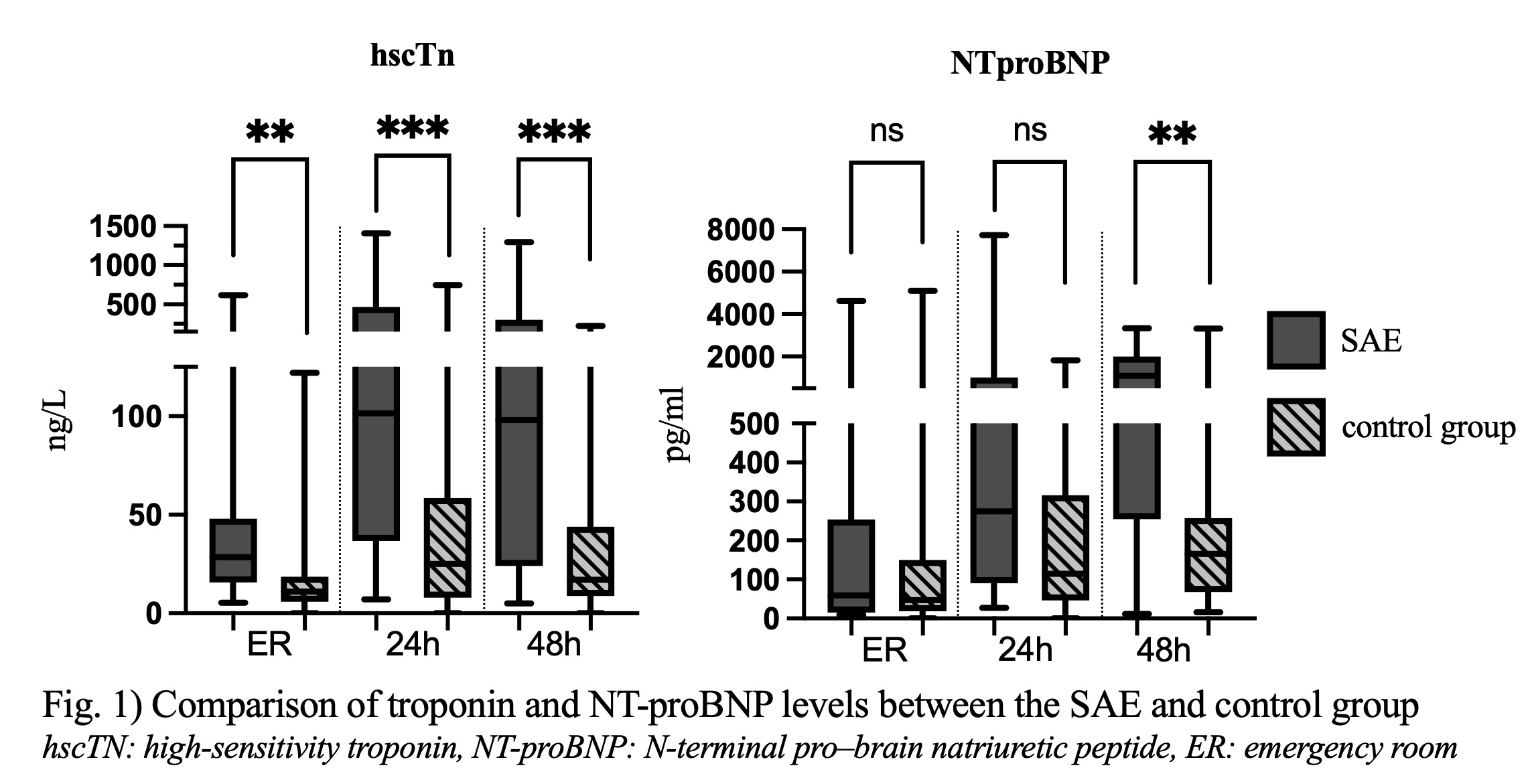
Eighteen patients (22.2%) developed SAE or fatal outcomes: 11 cardiac arrests (6 out-of-hospital, 5 in-hospital), 3 complete AV blocks, and 6 new-onset atrial fibrillation episodes; 5 patients died. SAE patients had significantly larger right ventricular end-diastolic diameters (29.9 ± 6.9 mm vs. 23.7 ± 5.5 mm; p < 0.01) and more frequent wall motion abnormalities (33,3% vs. 3,2%; p < 0.01). hscTn and NT-proBNP were elevated at admission and increased further within 48 h (hscTn: 696,2% vs. 102,7%; NTproBNP: +1610% vs. 223,5%; Fig. 1), whereas initial ECGs showed no discriminative value.
Conclusions:
Traumatic cardiomyopathy represents a distinct and underrecognized cardiac consequence of blunt trauma. Right ventricular dilation, new wall motion abnormalities, and rising cardiac biomarkers identify patients at increased risk of arrhythmia and mortality. Early imaging and biomarker-guided monitoring may improve detection and outcomes in trauma-associated cardiac injury.