Background: The systematic characterization of patient populations across different cardiomyopathy (CMP) phenotypes is essential for phenotype-specific risk stratification and treatment. The Translational Registry for Cardiomyopathies (TORCH) is a large-scale, prospective registry designed for the comprehensive study of CMPs. Our study reports the detailed baseline clinical and comorbidity spectrum of the TORCH and TORCH-Plus cohort stratified by CMP phenotype.
Methods: We analyzed the baseline patient cohort (N=4327) from the combined TORCH and TORCH-Plus studies. Patients were systematically stratified into CMP phenotypes, including Dilated Cardiomyopathy (DCM), Hypertrophic Cardiomyopathy (HCM), Cardiac Amyloidosis (CA), Left Ventricular Non-Compaction (LVNC), and Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC). Baseline demographics, cardiovascular risk factors, and functional status (NYHA class) were compared across these phenotype groups.
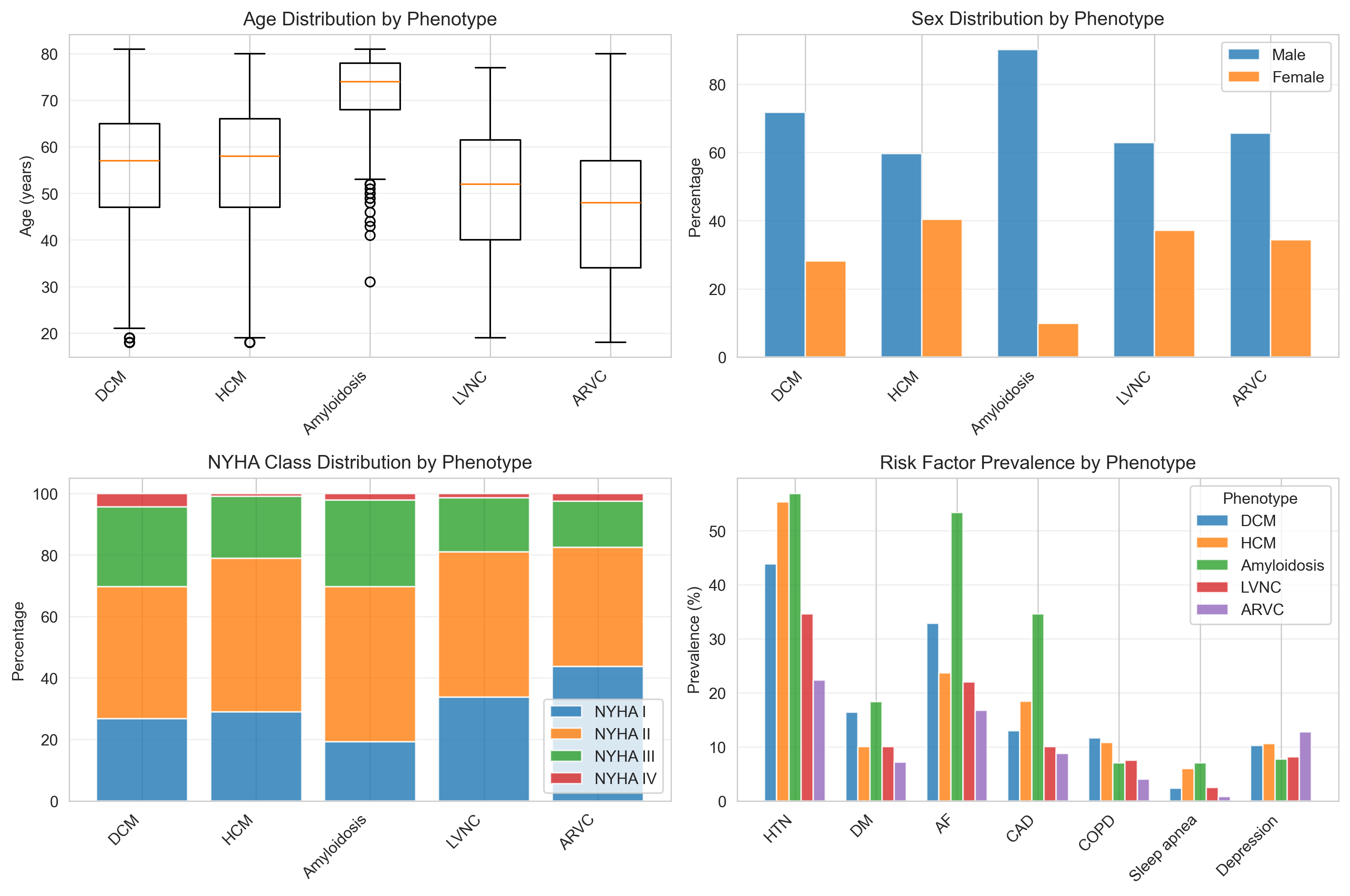
Results: The TORCH cohort (mean age 56.0 ± 14.2 years, 68.8% male) consists primarily of DCM (56.6%, n=2449) and HCM (30.3%, n=1311) patients, followed by CA (6.5%, n=283), LVNC (3.7%, n=159), and ARVC (2.9%, n=125). Significant differences in comorbidity profiles were observed between phenotypes. Patients with HCM exhibited a markedly higher prevalence of conventional cardiovascular risk factors at baseline, including hypertension (55.3% in HCM vs. 43.9% in DCM), dyslipidemia (39.5% in HCM vs. 30.8% in DCM) and sleep apnea (6.0% in HCM vs. 2.3%). Yet, the prevalence of Diabetes mellitus was higher in the DCM group (16.4% in DCM vs. 10.0% in HCM). Coronary artery disease (CAD) prevalence was highest in cardiac amyloidosis as expected by the older mean age at enrollment (34.6%), but was also significantly higher in HCM (18.4%) compared to DCM (13.0%), LVNC (10.1%), and ARVC (8.8%). Conversely, HCM patients demonstrated a significantly milder heart failure presentation at baseline compared to the DCM group. The prevalence of NYHA Class III/IV symptoms was 15.4% in HCM (vs. 27.9% in DCM). A history of heart failure (HF) decompensation was reported in only 5.0% of HCM patients (vs. 27.9% in DCM patients). The CA group was notable for the oldest mean age (70.8 ± 8.9 years) and a high prevalence of atrial fibrillation (53.4%).
Conclusion: The TORCH registry reveals distinct baseline comorbidity and functional profiles across cardiomyopathy phenotypes. Notably, the HCM population carried a higher burden of conventional cardiovascular risk factors (HTN, Dyslipidemia, CAD) while presenting with significantly milder heart failure symptoms compared to the DCM cohort. These findings underscore the differential role of risk factor management and the need for personalized approaches in patients with varying cardiomyopathy etiology.