BackgroundTargeting standard modifiable cardiovascular risk factors (SMuRFs) remains a cornerstone of secondary prevention after ST-segment elevation myocardial infarction (STEMI). However, patients presenting without SMuRFs – the so-called SMuRF-less phenotype – have occasionally been reported to experience higher long-term mortality, although findings have been conflicting. Evidence on their in-hospital outcomes is inconsistent, and data from German STEMI populations are scarce.
ObjectivesTo characterize SMuRF-less patients admitted within a German metropolitan STEMI network and to compare their clinical outcomes with those of patients presenting with SMuRFs.
MethodsThis multicentric metropolitan STEMI registry included patients registered between January 2024 and October 2025. SMuRF status was determined based on the presence of hypertension, diabetes mellitus, dyslipidemia, or smoking. The presence of at least one risk factor defined SMuRF positive patients. Outcomes included in-hospital mortality, cardiogenic shock (CS), angiographic culprit lesion, and stent implantation rate. Both unadjusted and adjusted binary logistic regressions were performed, adjusting for age (<65/≥65 years), sex, infarction type, and pre-existing coronary artery disease. A two-sided p-value <0.05 was considered statistically significant.
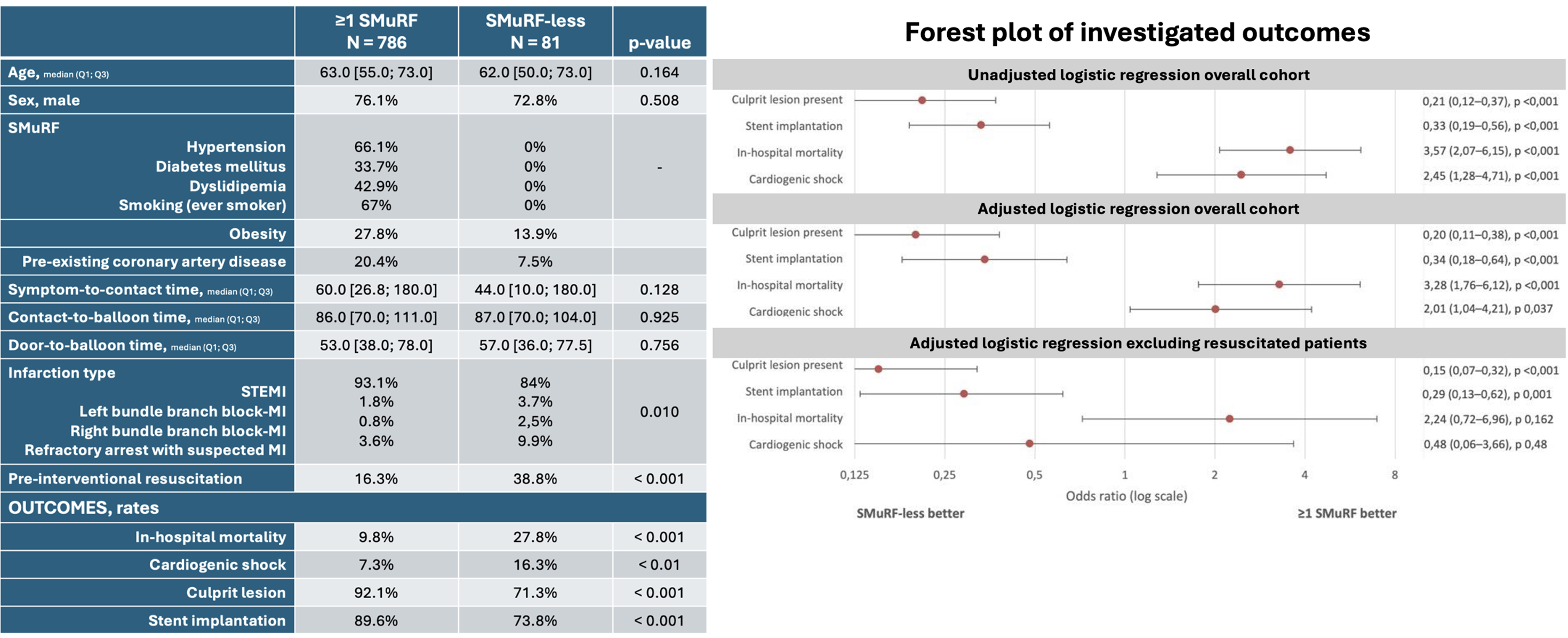
ResultsOf 1,128 recorded STEMI patients, 867 had complete SMuRF data. The groups were overall balanced except for differences in infarction type, resuscitation, pre-existing coronary artery disease (Table).
In unadjusted analysis, SMuRF-less patients showed higher odds of in-hospital mortality (OR 3.57, 95% CI 2.07–6.15, p<0.001) and CS (OR 2.45, 95% CI 1.28–4.71, p<0.01), but less frequent culprit lesions (OR 0.21, 95% CI 0.12–0.37, p<0.001) and stent implantations (OR 0.33, 95% CI 0.19–0.56, p<0.001) (Figure). In adjusted binary logistic regression analysis, these findings remained consistent (Figure).
Pre-interventional resuscitation emerged as the strongest independent predictor of mortality (OR 13.59, 95% CI 8.98–20.56) and was significantly more frequent among SMuRF-less patients. Sensitivity analysis excluding resuscitated patients demonstrated that differences in mortality and CS were no longer significant, while culprit lesion and stent implantation rates remained consistently lower in SMuRF-less patients (Figure). When resuscitation status was added to the regression model as further post-hoc adjustment, these observations remained consistent (data not shown).
Ultimately, SMuRF-less STEMI admissions less often had a culprit lesion and the need for urgent revascularization (71.3 vs. 92.1%, p<0.001).
ConclusionOutcome differences between SMuRF-less and SMuRF-positive STEMI admissions were mainly attributable to higher pre-interventional resuscitation rates in the SMuRF-less group, indicating possible survivorship or information bias. After adjustment, mortality and CS rates no longer differed significantly in this German STEMI network.
Remarkably lower rates of culprit lesions in SMuRF-less patients underscore the need for refined triage and more selective resource allocation in acute STEMI care.