AIMS: Acute right ventricular (RV) failure is a major concern after tricuspid valve replacement (TTVR) for severe tricuspid regurgitation (TR). The EVOQUE and LuX-Valve systems are the two most widely used devices. While symptomatic improvement after TTVR is well established, the acute RV response to complete TR elimination remains unclear. This study evaluated immediate and early changes in RV systolic function after TTVR.
METHODS: Consecutive patients undergoing EVOQUE or LuX-Valve TTVR between 2019 and 2025 were included in this multicentre study. Intraprocedural RV performance was assessed by transoesophageal echocardiography, while baseline and discharge parameters were obtained by transthoracic echocardiography. RV contractility (end-systolic elastance, Ees) and afterload (arterial elastance, Ea) were derived from non-invasive pressure–volume loops combining invasive hemodynamics with CT-based volumetry.
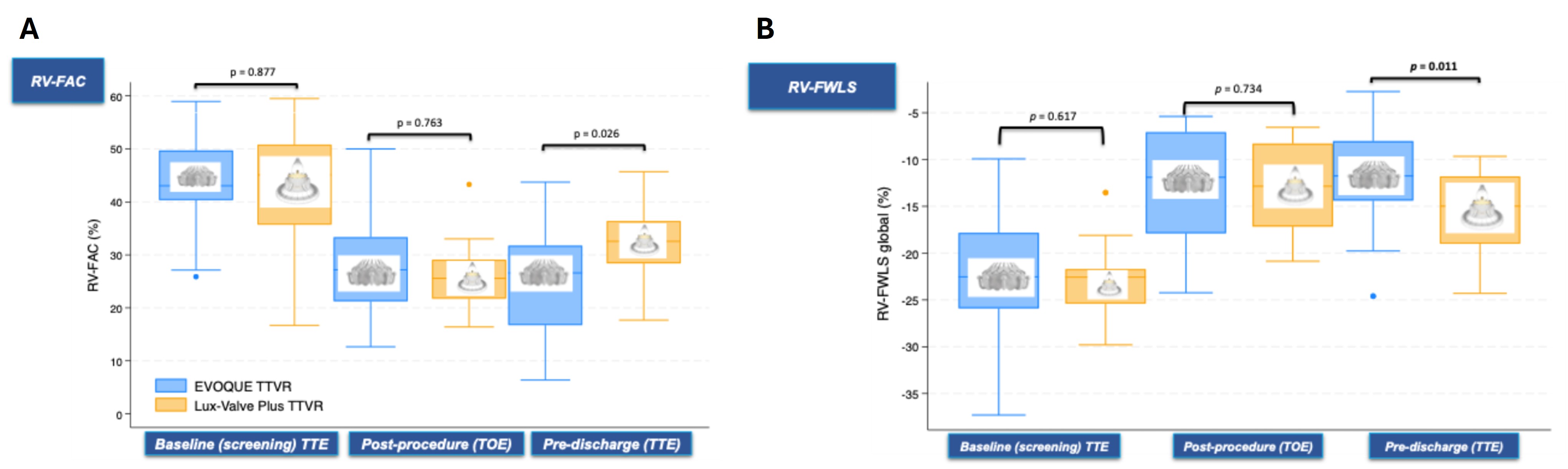
RESULTS: Sixty-three patients (median age 78 years [IQR 73–84], 73 % female, 84 % NYHA ≥ III) were analysed. Both valve types achieved near-complete TR elimination (grade 5 [IQR 4–5] to 1 [IQR 0–1], p<0.001). Patients treated with LuX-Valve had lower baseline RV ejection fraction (39 vs 50 %, p=0.003) and Ees (0.30 vs 0.35 mmHg/mL, p=0.045), while Ea was similar (p>0.05). Immediately after implantation, RV free-wall strain (FWS) and fractional area change (FAC) declined (ΔFWS −11.2 % [−16.0 to −7.8], ΔFAC −12.9 % [−18.5 to −7.7], both p<0.001) without change in RV size (ΔRVEDA −1.4 cm², p=0.27). The magnitude of decline did not differ between valve types (p>0.05).
At discharge, EVOQUE patients exhibited a persistently lower RV FAC (−19.3 % vs −13.5 %, p=0.024), whereas partial recovery of RV FWS and FAC was seen after LuX-Valve implantation (Figure 1A,B). In the EVOQUE cohort, ΔFWS correlated with baseline Ees (r = 0.44, p = 0.043), indicating a stronger reduction in patients with lower contractile reserve. At a median follow-up of 456 days [IQR 282 – 666], 12 (26 %) patients treated with the EVOQUE valve and 1 (6 %)treated with the Lux valve died. Neither early reduction in RV FWS nor FAC was associated with 2-year survival (p>0.05).
CONCLUSION: TTVR results in a transient reduction of RV systolic function, most pronounced in EVOQUE recipients with limited baseline contractility. Early recovery of RV longitudinal and radial function occurred predominantly after LuX-Valve implantation. The lack of association between immediate RV functional decline and mid-term survival suggests that acute reductions in RV performance are well tolerated in appropriately selected patients. Importantly, baseline RV contractility quantified by Ees may serve as a useful screening parameter to identify patients at increased risk of very early RV failure.