Introduction: Wolff-Parkinson-White (WPW) syndrome as a congenital cardiac preexcitation syndrome is associated with symptomatic arrhythmia even in young patient and characterized by a short PR-Interval, prolonged QRS-Complex and Delta wave on ECG due to abnormal cardiac conduction through an accessory pathway. In some patients the Delta wave and short PR interval are not notable during exercise.
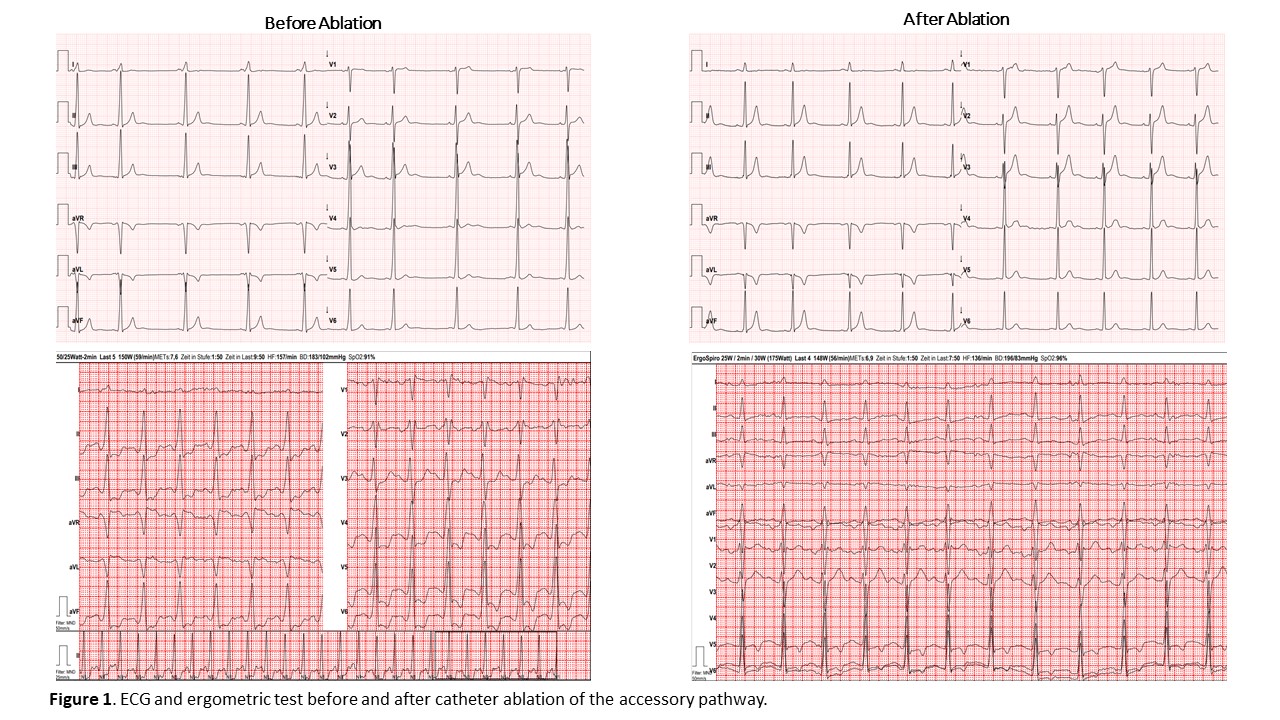
Case Report: A 19 year old asymptomatic male athlete in competitive sport without any medical history was referred to our hospital cause a preventive stress test before starting police career has shown significant ST-segment depression in the precordial and inferior leads. Therefore, a spiroergometry was reproduced with descending ST-segment depression after 100 Watt until a maximum exercise of 223 Watt. The 12-channel resting ECG demonstrated a bradycard sinus rhythm with 56 bpm, PR-Interval of 105 msec, QRS-Complex of 110 msec. A closer look reveals a small Delta wave in I, the inferior leads and V5 to V6. In the echocardiography no significant findings were observed up to a small mitral valve regurgitation. The cardiac MRI ruled out a cardiomyopathy, acute myocarditis and fibrosis. During CT-Angiography of coronary arteries an atypical variant of ramus circumflexus was noted without any reasonable coronary ischemia. Furthermore, an electrophysiological examination was planned to check preexcitation especially in presence of the short PR-Interval although no previous arrhythmic episodes were reported. According to class IA indication (ESC guidelines) a left-lateral located accessory pathway was ablated successfully during catheter ablation. The following 12-channel resting ECG showed a sinus rhythm with 61 bpm, PR-Interval of 124 msec and QRS-Complex of 106 msec. Three months later the athlete was tested again with ergometry without significant repolarization disorders at a maximum exercise of 258 Watt compared to the deep ST-segment depression of the previous examination.
Discussion: During stress test, like ergometric test, significant ST-segment depression, which normally are associated with ischemia, are observed in 49% of the patients with Wolff-Parkinson-White syndrome. Due to accessory pathways these findings may have another meaning than in patients without preexcitation. Therefore, ST-segment depression during stress test in the presence of preexcitation should be considered as false positive, especially in asymptomatic young patients. These ST-segment depression in patients with preexcitation are affiliate to different myocardial depolarization and following repolarization through an accessory pathway.
Conclusion: In patients with Wolff-Parkinson-White syndrome ergometric stress test may lead to false positive results and should not be used for diagnosis of coronary artery disease.