Background
Comparative data on fatal complications associated with catheter ablation for atrial fibrillation (AF) using different energy sources remain limited.
Objective
The aim of the TiFFANY (Total number of Fatal adverse events Following Atrial fibrillation ablatioN from an FDA mandatory reporting sYstem) -Fire and Ice study was to analyse reported deaths after radiofrequency (RF) and cryothermal AF ablation, as documented in the Manufacturer and User Facility Device Experience (MAUDE) database of the FDA.
Methods
The MAUDE database was systematically searched for reports of death following AF ablation using RF or cryothermal energy between 2014 and 2024 using standardised terms. All types of AF ablations were included. All reports were reviewed by two reviewers, with discrepancies resolved by a third. Duplicate reports were excluded. When available, data cited from referenced literature were extracted. Event characteristics, diagnostic, and treatments were summarized descriptively and compared between groups using Fisher’s exact test or the Mann–Whitney U test, as appropriate.
Results
A total of 282 deaths were identified: 151 (53.5%) after RF ablation and 131 (46.5%) following cryothermal ablation.
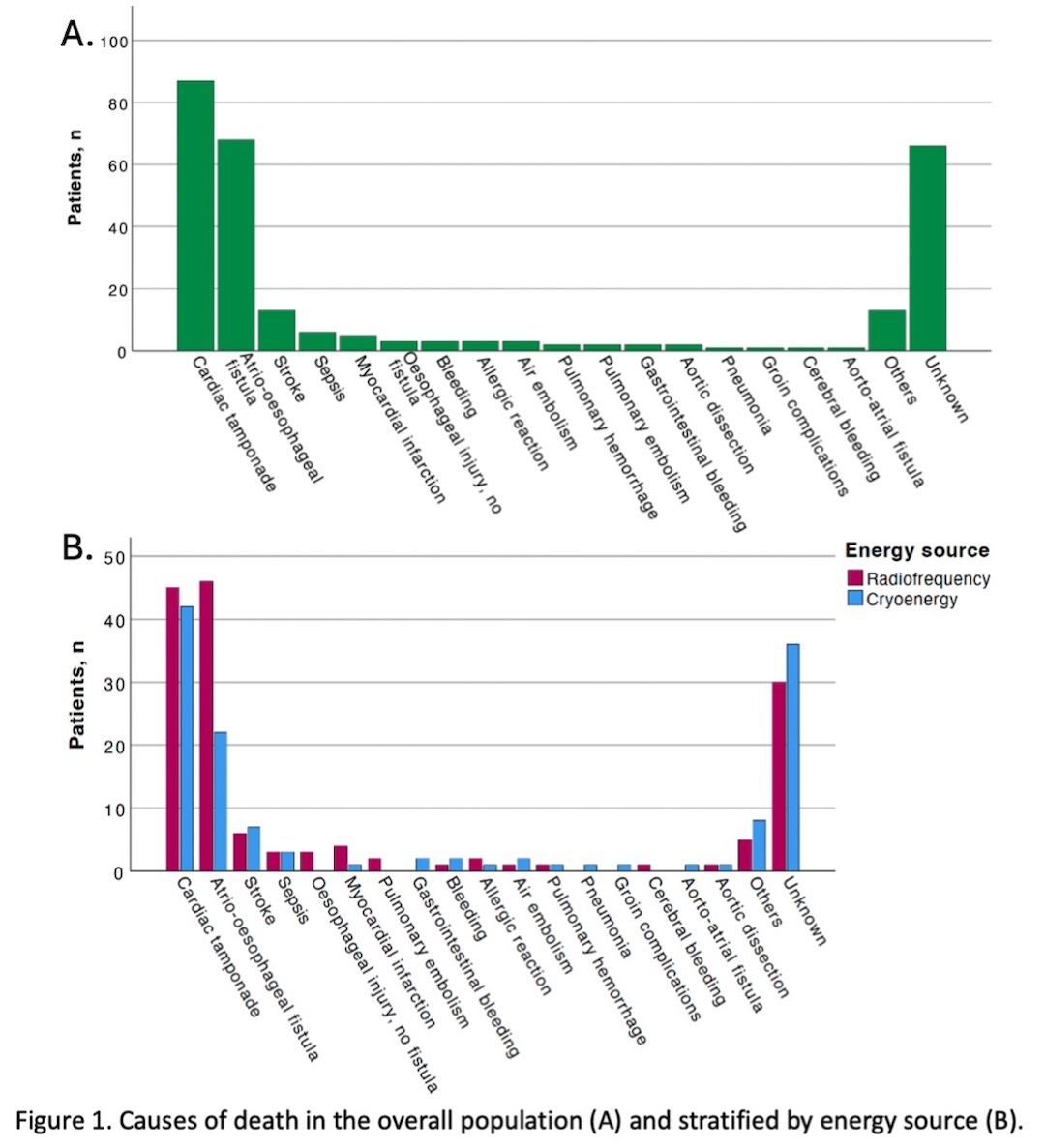
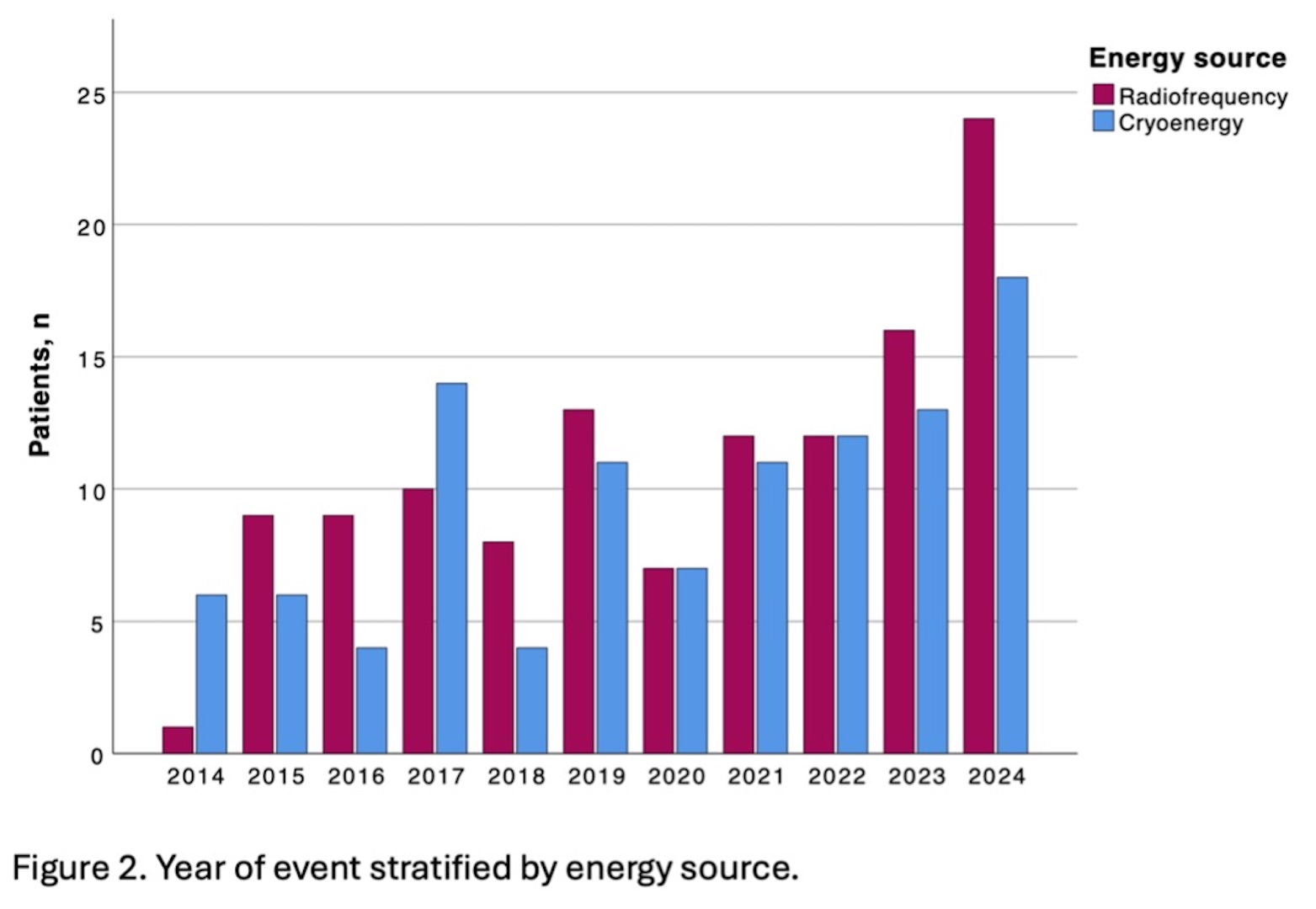
The predominant cause of death was oesophageal fistula in the RF group (38.0%;46/121 RF deaths) and cardiac tamponade in the cryothermal group (44.2%; 42/95 cryothermal deaths) (Figure 1). Most fatalities occurred during the latter half of the study period (62.0% for RF and 59.4% for cryothermal, Figure 2). Most reports originated from the United States (RF 49.6%, cryothermal 54.0%).
A device-related problem was reported in 2.1% (3/140) of RF and 5.4% (6/111) of cryoenergy cases (p = 0.190). Median time to death was 1 (0–7) day after RF and 1 (0–19.5) day after cryothermal ablation (p = 0.244). Among reports containing symptom data (40.1%), the most frequently reported symptoms were hypotension (50.9% in RF vs. 47.5% in cryothermal ablation), neurological deficits (30.2% vs. 21.3%), and fever (18.9% vs. 21.3%) (all p>0.05).
Diagnostic modalities were available in 48.3% (73/151) of RF and 48.1% (63/131) of cryothermal cases, most commonly echocardiography (60.3% vs. 52.4%) and computed tomography (26.0% vs. 28.6%). Treatment information was available in 53.5% of reports, with interventional management performed in 62.3% (48/77) vs. 70.3% (52/74) (p=0.390) and surgical treatment in 40.3% (31/77) vs. 52.7% (39/74) of RF and cryothermal cases (p=0.144), respectively.
Based on estimated global procedural shares (≈70% RF, 30% cryothermal), the relative reporting proportion of deaths appeared roughly twofold higher after cryothermal ablation.
Conclusions
Cardiac tamponade and oesophageal fistula represent the leading causes of death after AF ablation. As MAUDE lacks procedural denominators and may present reporting bias, the findings should be interpreted as reporting patterns rather than incidences. However, despite comparable absolute numbers of reported fatalities, the relative reporting proportion under denominator assumptions (adjusted for procedural prevalence) was approximately twofold higher after cryothermal ablation.