Background
Sodium–glucose cotransporter 2 inhibitors (SGLT2i) have been shown to reduce the risk of heart failure hospitalization in high-risk populations. However, patients with aortic valvular heart disease were largely excluded from major clinical trials, and recent studies have mainly focused on individuals with aortic stenosis (AS) undergoing transcatheter aortic valve replacement (TAVR). Consequently, the potential impact of SGLT2i therapy on mortality in an unselected, real-world population of patients with aortic valve disease remains unclear.
Methods
Data were obtained from TriNetX, a global federated network of anonymized electronic health records used for large-scale real-world analyses. A cohort of patients with newly diagnosed aortic valve disease, including incident cases of aortic stenosis (AS) and/or aortic regurgitation (AR) was investigated. In addition, patients with a history of transcatheter (TAVR) or surgical (SAVR) aortic valve replacement were analyzed as separate prespecified subgroups. Within this cohort, we assessed the association between newly initiated SGLT2i therapy and all-cause mortality, compared with patients without any SGLT2i exposure. Extensive propensity score matching was performed for age, sex, ethnicity, socioeconomic status, diabetes, heart failure, obesity, coronary artery disease, atrial fibrillation, stroke, malignancy, alcohol use, and mood or anxiety disorders.
Results
Among 1,437,117 patients with aortic valve disease, after exclusions and matching, five matched cohorts were defined: 13,166 patients with AS, 13,767 with AR, 4,140 with combined AS + AR , as well as 3,800 post-TAVR and 2,192 post-SAVR. SGLT2i use was associated with a 32.6% reduction in all-cause mortality among AS patients (HR 0.674; 95% CI 0.637–0.713; p < 0.0001), a 22.7% reduction after TAVR (HR 0.773; 95% CI 0.689–0.867; p < 0.0001), and a 37.6% reduction after SAVR (HR 0.624; 95% CI 0.507–0.769; p < 0.0001). Similarly, in patients with AR, SGLT2i therapy was associated with a 35.1% lower mortality (HR 0.649; 95% CI 0.610–0.791; p < 0.0001), and in combined AS + AR cases with a 22.3% lower mortality (HR 0.777; 95% CI 0.689–0.876; p < 0.0001). All covariates were well balanced (SMD < 0.1), and proportional hazards assumptions were met (global tests p > 0.2). Sensitivity analyses confirmed the main findings, and the negative control outcome (burns) was not significant (p = 0.17).
Conclusions
In this large, real-world cohort, SGLT2 inhibitor therapy was associated with a significant reduction in all-cause mortality among patients with aortic valve disease, independent of diabetes or heart failure status. While randomized controlled trials are warranted to confirm these findings, the results support consideration of SGLT2i as an adjunctive therapy in patients with aortic valve disease.
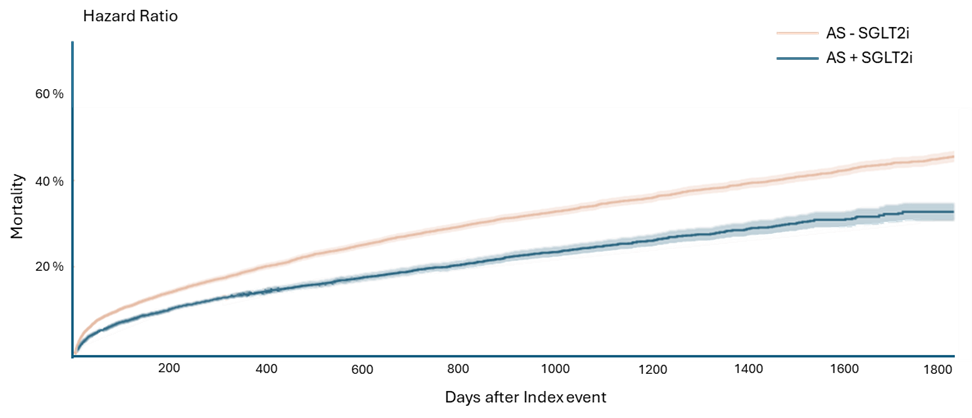
Figure 1: All-cause mortality in aortic stenosis according to SGLT2-inhibitor use



