Background
Pulsed-field ablation (PFA) has recently emerged as a new modality for pulmonary vein isolation (PVI) in the treatment of atrial fibrillation (AF). Early studies indicate that PFA offers a favorable safety profile, while its rhythm-control efficacy has been shown to be comparable to thermal ablation strategies. While targeting the pulmonary vein (PV) antrum is critical for successful isolation, lesion extension has been observed to be greater with PFA than with thermal energy sources. It is possible that larger lesions reduce left atrial (LA) function after PFA-based PVI. Speckle-tracking echocardiography is a widely available, non-invasive, and validated method for assessing LA function. This analysis compared LA function at 12 months after a successful first PVI using PFA or the thermal energy sources radiofrequency (RFA) and cryoballoon (CBA) ablation.
Methods
Consecutive patients undergoing first-time PVI using PFA, CBA, or RFA were prospectively enrolled into the TRUST registry (NCT05521451). Transthoracic echocardiography was performed at baseline and at 12-month follow-up. Patients were included if in sinus rhythm at both examinations. LA function was quantified by LA reservoir strain (LASr), conduit strain (LAScd), contraction strain (LASct), and LA emptying fraction (LA-EF). Paired and between-group analyses were performed using non-parametric tests for repeated measures.
Results
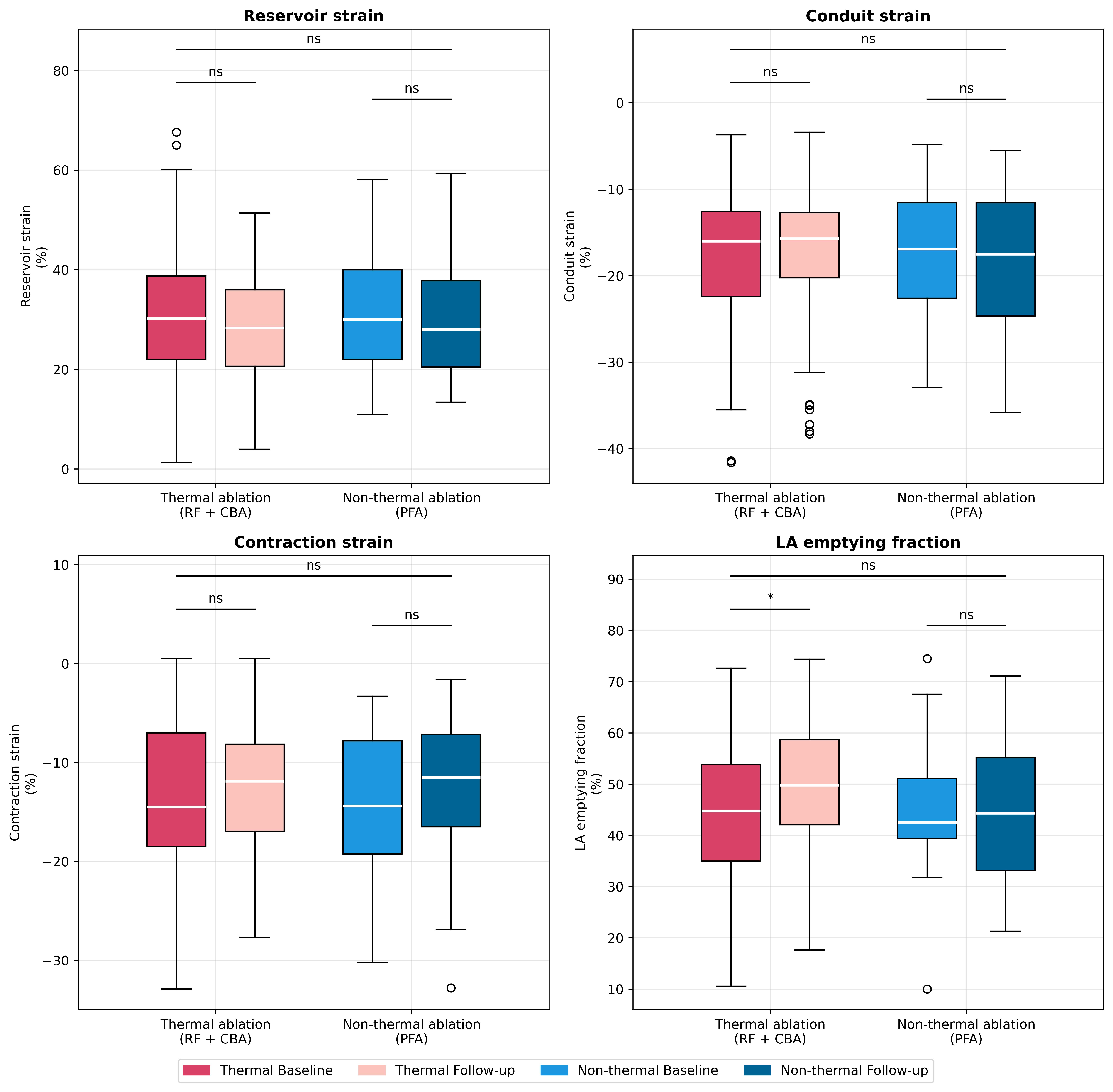
Among 142 patients (35% female; median age 64 [56–72] years), 47 (33%) underwent PFA and 95 (67%) thermal ablation (CBA 69, RFA 26). Posterior wall isolation was not attempted in any procedure. Baseline left ventricular function and LA parameters were preserved and comparable between groups. At 12 months, no between-group differences for delta changes were observed between PFA and thermal ablation for LASr (p=0.32), LAScd (p=0.17), LASct (p=0.89). or LA-EF (p=0.23). Within the thermal ablation group, LA-EF increased by 6.4% [-7.2%, 16.5%] (p=0.02) from baseline LA-EF while no difference was observed after PFA (0.36% [-10.9%, 11.0%]; p=0.23). Further multivariate and subgroup analyses will be presented.
Conclusions
Left atrial function is preserved one year after successful pulmonary vein isolation across all ablation modalities, including unchanged LA reservoir, conduit, contraction strain, and LA emptying fraction, at levels comparable to thermal ablation. The moderate sample size and single-center design warrant verification in larger multicenter cohorts to confirm these results and further elucidate atrial remodeling patterns after non-thermal ablation.