BackgroundCurrent atrial fibrillation guidelines recommend rhythm control to improve AF-related symptoms in patients with AF. In addition to patient-reported questionnaires and symptom scales, assessment of patients’ physical activity and related physiological parameters via consumer smartphones and smartwatches may provide additional information on patients’ health state. Daily physical activity significantly impacts health outcomes including cardiovascular disease, mental health, and all-cause mortality. While activity trackers are successfully used in epidemiological research, they are rarely used to estimate physical activity in patients with AF. Here, we report an early feasibility study conducted within the Long-term Outcome and Predictors for Recurrence after Medical and Interventional Treatment of Arrhythmias (TRUST) study, to evaluate whether daily step counts can be remotely ascertained before and after first-time pulmonary vein isolation (PVI).
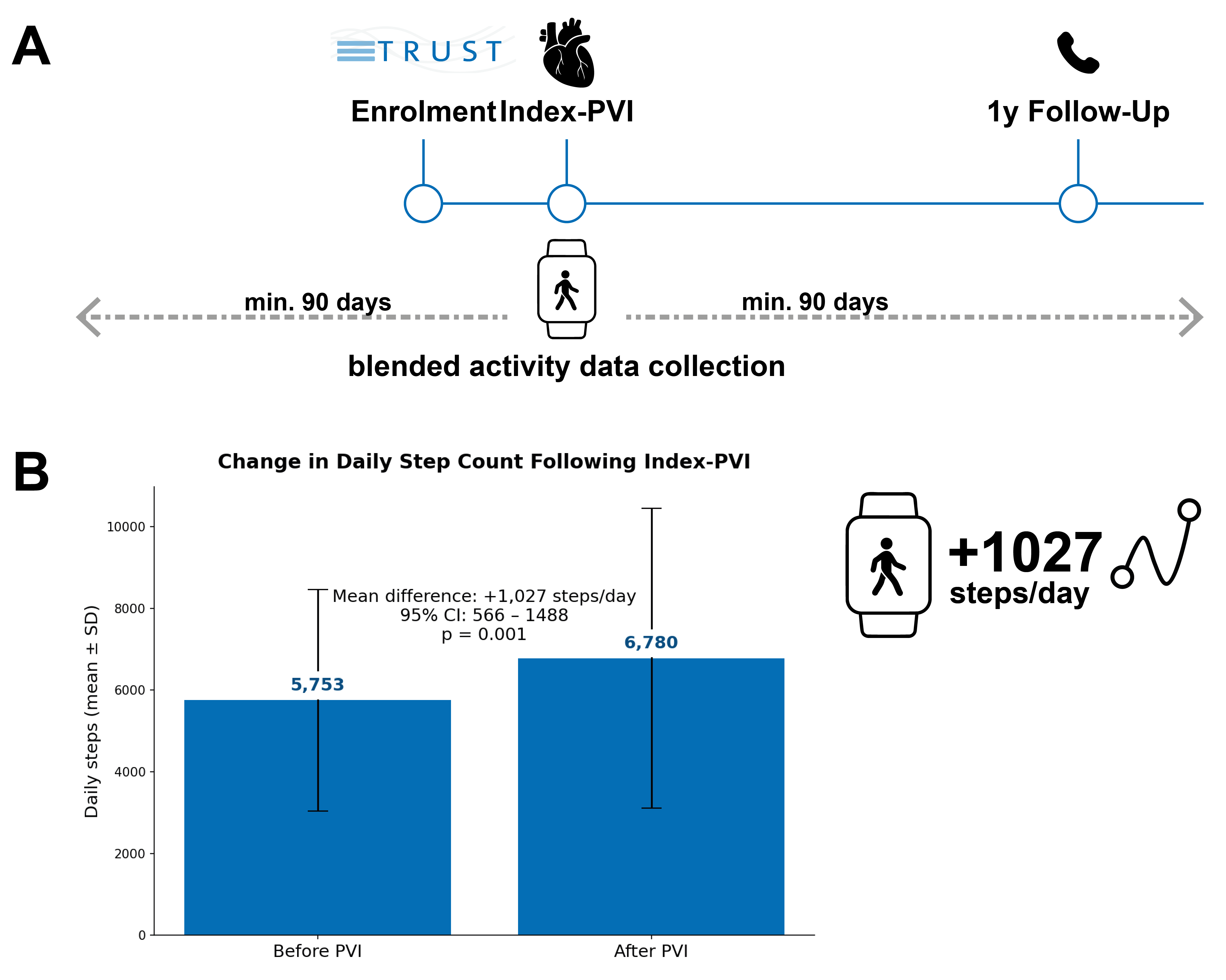
MethodsThis secondary analysis included patients with diagnosed AF who underwent first-time PVI after their enrolment in TRUST (NCT) and who reported owning an eligible smartphone. Patients willing to contribute continuous smartphone-collected activity data were guided through the necessary steps to export health data from their devices to a secure web-based data collection system hosted at and by the study center. Collected data included the daily step count and, for smartwatch carriers, daily mean, maximal and minimal resting heart rate, atrial fibrillation episodes, sleep episodes, mean, maximal and minimal blood oxygen, and maximal oxygen consumption (VO2max). All parameters were manufacturer-validated; the AF detection algorithm has FDA clearance and CE marking. Only patients with ≥90 consecutive monitoring days both before and after PVI and without >10-day gaps were included.
ResultsTo date, data from 105 patients (32 female (31%); median age 67.0 [59;74] years; 40% persistent atrial fibrillation; mean CHA2DS2-VA score 1.6±1.3; mean AFEQT score upon enrolment 75.2 ± 20.7; EQ-VAS upon enrolment 71.9±18.2) were retrieved with 1866.1±725.0 monitoring days per patient, of which 942.2±523.5 monitoring days were recorded before and 923.0±413.5 after the individual procedure dates. Out of 105 patients, 90 (86%) provided data from at least 90 continuous days both prior to and post PVI. Of the patients in this analysis cohort, 52/90 (58%) were regular smartwatch carriers for whom extended monitoring data were available. Among these patients, atrial fibrillation burden data were available from 30/52 (58%) patients. Daily step count increased from 5753±2705 to 6780±3666 after PVI (mean increase +1027 steps/day, 95%-CI 565.54 -1488.36; p=0.001). Patients with a greater increase in daily activity were more likely to improve by at least one New York Heart Association (NYHA) functional class at follow-up (OR 0.75, 95% CI [0.58-0.97]; p=0.026).
ConclusionsRemote ascertainment of daily step counts was feasible in patients undergoing a first AF ablation. Most participants contributed analyzable data over multi year periods with minimal days lacking data. Preliminary analyses suggest increased physical activity after ablation.