Background and Aims
This subgroup analysis of the multicentric, epidemiological non-interventional SCD-PROTECT study aims to specifically assess the risk for sudden cardiac death (SCD) due to ventricular arrhythmia in patients with newly diagnosed tachycardiomyopathy (TCM) during the phase of up-titration of guideline-recommended medical therapy. For the first time, circumstances of appropriate treatments were described in detail.
Methods
The SCD-PROTECT study analyzed 19.598 consecutively enrolled patients between 18 and 80 years of age in Germany, that used a WCD as protection against SCD. For this subgroup analysis, all patients with TCM were included and assessed. The primary endpoint was the incidence rate of SCA due to ventricular arrhythmia documented by appropriate WCD shocks. Secondary endpoints included incidence of inappropriate WCD treatments, mortality, and frequency of adverse events. Furthermore, appropriate treatments were assessed in detail.
Results
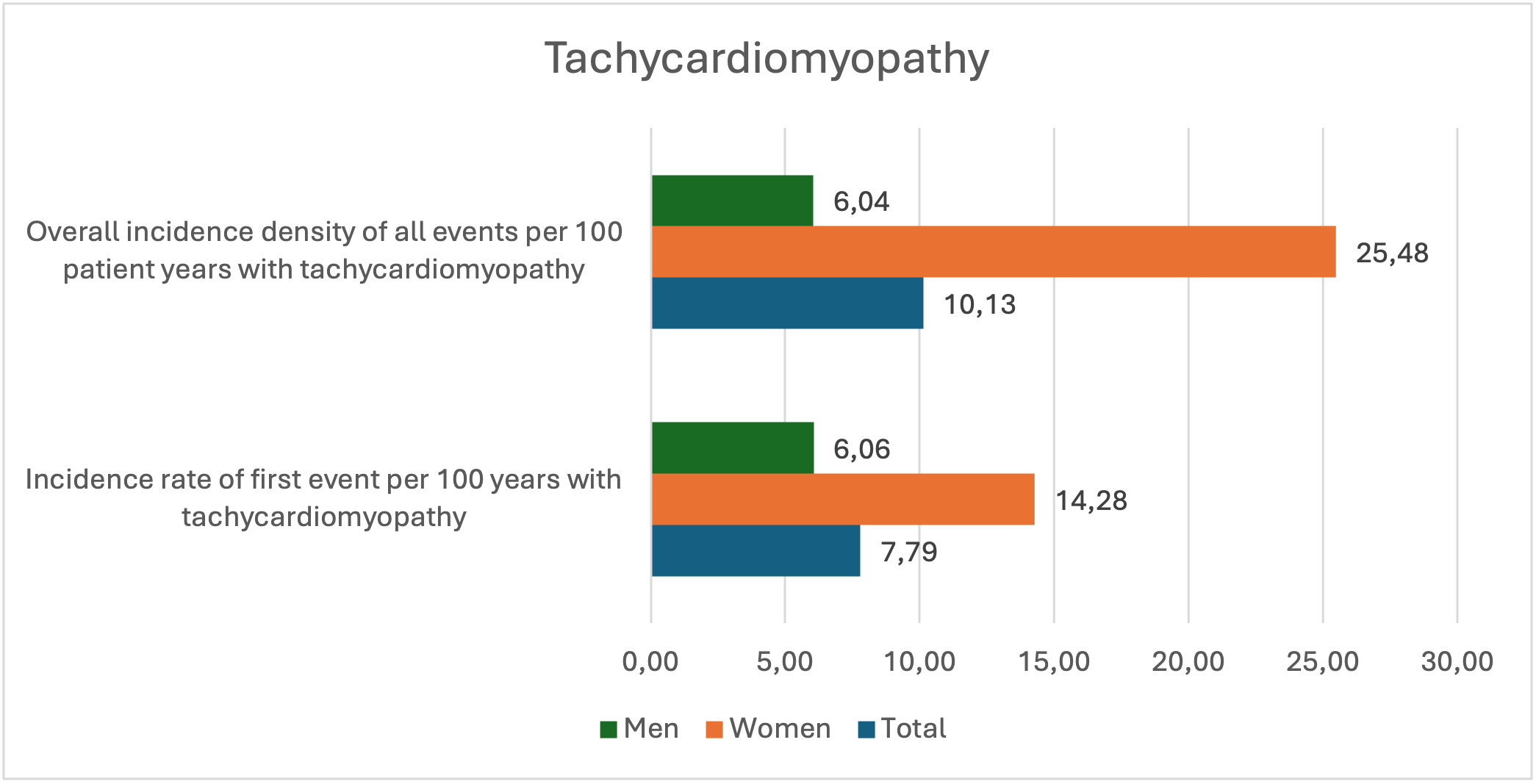
1,056 patients with TCM were analysed. Mean age was 63.3±11.0 years and female patients accounted for 21.5% of patients. The incidence rate of first appropriate treatment in all TCM patients was 7.79 per 100 patient-years (95%CI 4.15-13.32), i.e. 6.06 per 100 patient-years (95%CI 2.62-11.95) in men and twice as high in women with 14.28 per 100 patient-years (95%CI 4.64-33.32). The overall incidence density of appropriate treatments was 10.13 per 100 patient-years (95%CI 5.90-16.22) in the total group, 6.04 per 100 patient-years in men (95%CI 2.61-11.90), and 25.48 per 100 patient-years in women (95%CI 11.65-48.36), respectively.
Women with appropriate treatment tended to be older (mean 72.0±5.5 years) than women without (66.4±10.2 years, p=0.21) and had a numerically a lower mean left ventricular ejection fraction (LVEF) at WCD fitting with 22.2±6.3% vs. 27.7±8.9% (p=0.17). LVEF at end of WCD use was significantly lower for patients with appropriate treatment compared to patients without (mean 34.2±6.8% vs. 42.8±9.4%, p=0.04) and the percentage of patients with ICD implantation was slightly higher (66.7% vs. 17.9%, p=0.38). WCD recorded data of patients with appropriate WCD treatment are reported in the accompanying table.
Eight inappropriate treatments (0.6%) occurred in seven patients. LVEF at fitting of the WCD was 26.6±8.6% and improved to 42.7±9.5% at end of WCD use. 18.4% of all patients with TCM (17.7% of men and 21.2% of women) were implanted with an ICD at end of WCD use. Three patients (0.3%) died.
Conclusions
Patients with TCM have a substantial risk for SCD in the first months after diagnosis. Women, which were considerably older at study enrolment, showed a more than doubled risk compared to men.
Figure 1: Incidence rate of first WCD event and overall incidence density in total and by gender