Background
The factors determining hemodynamic stability of ventricular tachycardia(VT)in patients with structural heart disease are not fully understood. Previous studies have shown that an inadequate sympathetic response is associated with poorer hemodynamic tolerance. However, these data were obtained from patients undergoing catheter ablation (CA) under general anesthesia with dopamine preloading. To date, no data exist on VT ablation under deep sedation(DS) with propofol and fentanyl.
Purpose
To evaluate the sinus rate(SR) response during monomorphic VT in patients undergoing CA under DS.
Methods
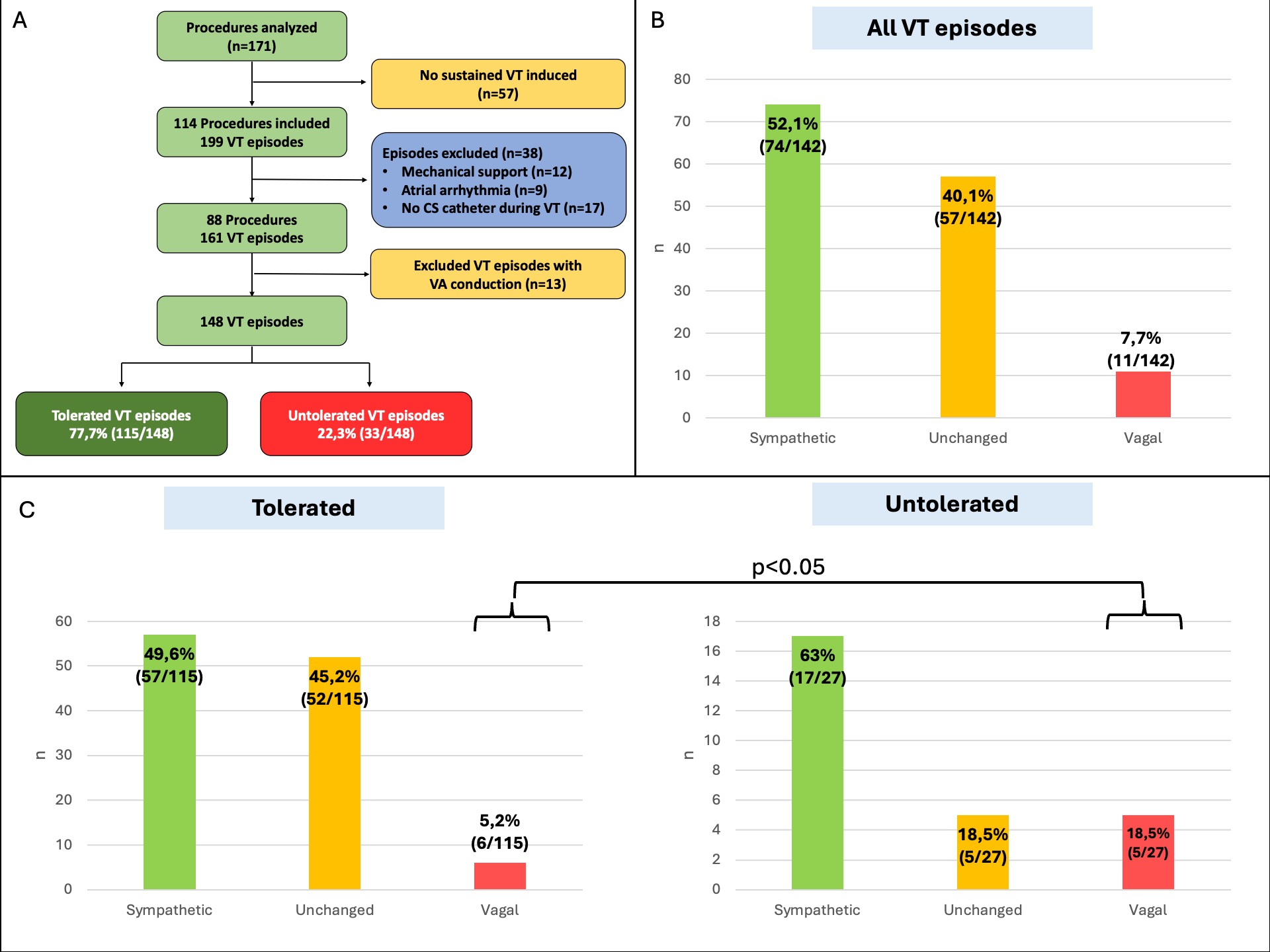
This retrospective single-center study included all scar-related VT CA procedures performed under DS between 01/2022 and 09/2025(n=171). After excluding 57 procedures without VT induction, 9 with atrial arrhythmias, 12 with mechanical support, and 17 without atrial signal recording during VT, 87 procedures were analyzed. After additional exclusion of 13 episodes with 1:1 ventriculo-atrial conduction, 148 VT episodes were included(Fig.1A). Autonomic response was assessed by measuring SR cycle length (CL) on the coronary sinus catheter before and after VT induction (at 5,10,15,30, and 60s). Three response types were defined: sympathetic (SR increase ≥5 bpm), vagal (SR decrease ≥5 bpm), and unchanged at 30 s. Untolerated VT was defined as VT requiring cardioversion within 150 s due to hemodynamic instability.
Results
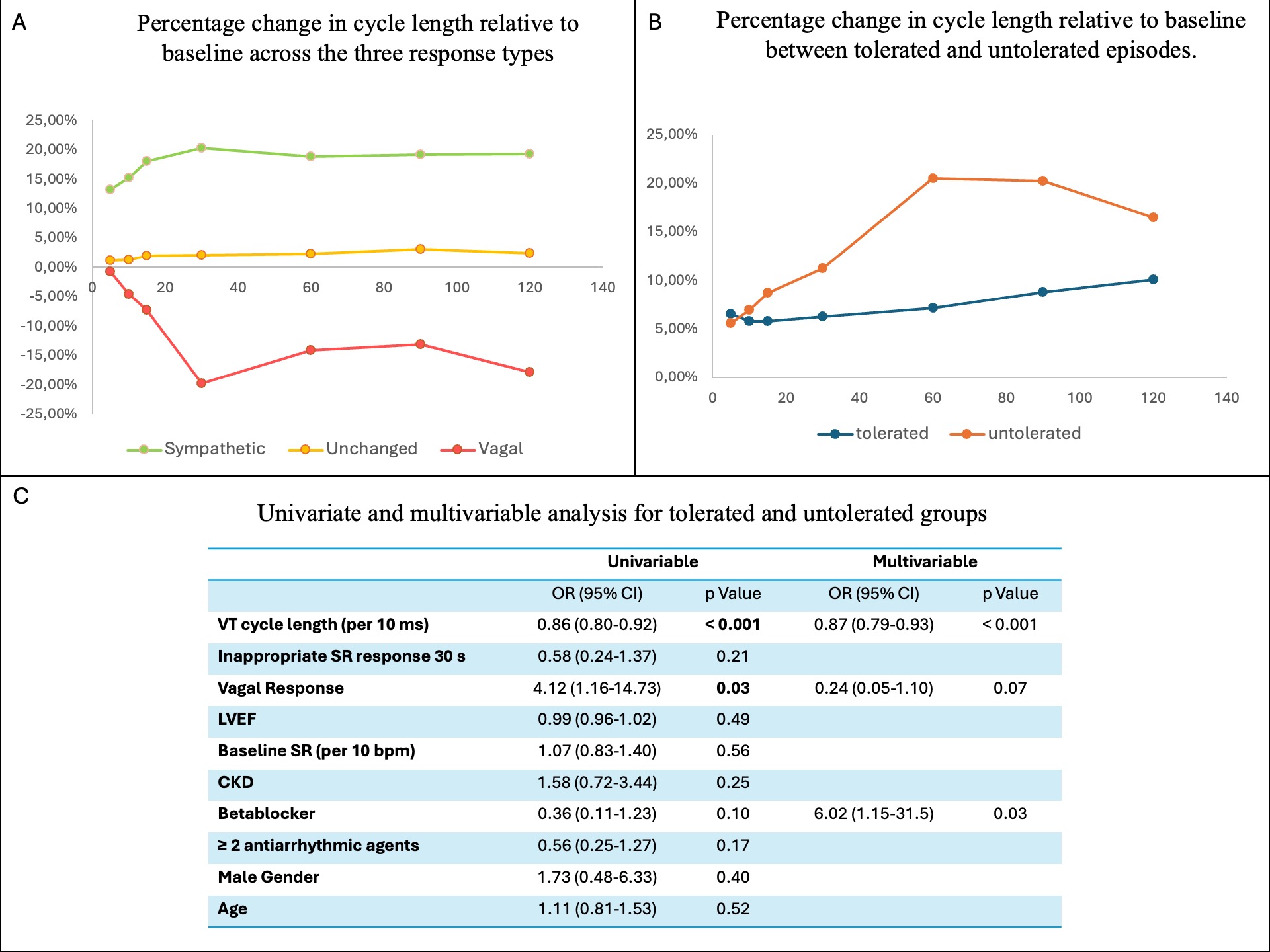
Eighty-seven procedures were included. Median age was 64 years, 15% were women, 38 patients (43%) had LVEF <30%, 59 (52%) ischemic cardiomyopathy, 18% presented with VT storm, and 39% received ≥2 antiarrhythmic drugs. In total, 148 VT episodes were analyzed, 115 (78%) tolerated and 33(22%) untolerated. Tolerated episodes lasted longer (503 vs 57 s, p<0.001). Among all episodes, 74 (52%) showed a sympathetic, 57(40%) an unchanged, and 11(8%) a vagal SR response (Fig.1B). Relative to baseline CL, the median SR change at 30 s was +20.3% for sympathetic, -19.8% for vagal, and +2.0% for unchanged responses (Fig.2A). Vagal responses were more frequent in untolerated than tolerated VT (18.5% vs 5.2%, p<0.05)(Fig.1C). Despite this, untolerated VT episodes showed a trend toward greater SR CL change than tolerated ones at 15 (+8.7% vs +5.8%), 30 (+11.2% vs +6.3%), 60 (+20.5% vs +7.1%), and 90 s (+20.2% vs +8.8%) (Fig.2B). In multivariable logistic regression, shorter VT CL remained independently associated with VT intolerance (OR 0.87 per 10 ms decrease, p<0.001). Beta-blocker therapy was also associated with VT intolerance (OR 6.02, 95% CI 1.15–31.5, p=0.03). Vagal response showed a trend toward association (OR 0.24, p = 0.07) but did not reach statistical significance.
Conclusion
Almost half of all VT episodes failed to accelerate the SR during VT. Besides VT CL and beta-blocker use, a vagal SR response was associated with hemodynamic intolerance of VT in patients undergoing ablation under DS without dobutamine preloading.