Introduction
Deep intramural substrates may not be accessible using conventional unipolar endocardial or epicardial ablation. Bipolar radiofrequency ablation (B-RFA) enables creation of deeper lesions by delivering energy between two catheters positioned on opposite sides of the septum or within the coronary venous system. We evaluated the safety and efficacy of bipolar ablation when one catheter was positioned in the free epicardial space, presenting the largest cohort of patients who underwent bipolar endo-epicardial ablation for ventricular tachycardia (VT).
Methods
All procedures were performed under deep sedation with fentanyl and continuous propofol infusion. Catecholamines were administered if hypotension occurred. Epicardial access was achieved via subxiphoid puncture with a Tuohy needle under fluoroscopic guidance. Electroanatomical mapping of endocardium and epicardium was performed with either EnsiteX or CARTO3. The active ablation catheter (AC) was QDot for CARTO and TactiFlex for Ensite; the return catheter (RC) was ThermoCool, connected to the generator’s indifferent port via a Dr. Futyma Bipolar Ablation Adapter instead of a dispersive patch. Bipolar ablation was used when diastolic potentials were absent on one side despite high-density mapping. Epicardial applications were delivered >5 mm from coronary arteries and outside phrenic nerve capture zones.
Results
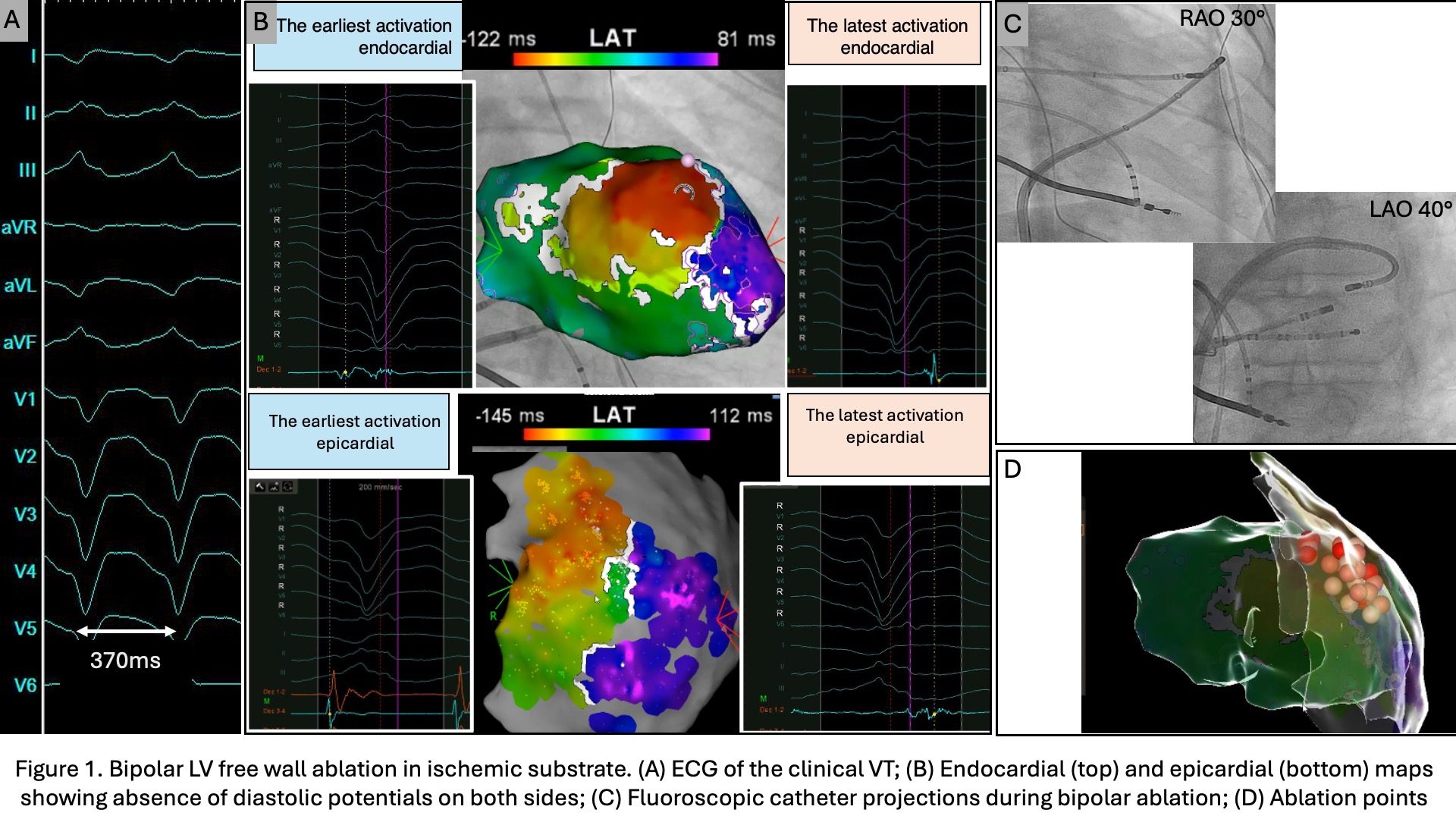
Nine procedures in seven male patients were analyzed (median age 65 years, IQR 60–74). Four had ischemic, two dilated, and one arrhythmogenic cardiomyopathy; four presented with VT storm. Median LVEF was 30% (IQR 25–37.5). All received beta-blockers, and two (29%) were on amiodarone. Four procedures (44%) were first-time, five were repeat ablations after failed unipolar procedures. Endocardial access was transseptal in all. Median procedure duration was 186 min (IQR 177–205) and fluoroscopy 19 min (IQR 14–22). Unipolar ablation (8/9 cases) was performed at 40–50 W with 28 min (IQR 20.5–41.5) total time and 30 lesions (IQR 23–41). Bipolar ablation (20–30 W) lasted 19 min (IQR 17–23) with 18 lesions (IQR 14–22), baseline impedance 150 Ω (IQR 130–170), impedance drop 17 Ω (IQR 15–19), and intercatheter distance 15 mm (IQR 13–18). Ablation sites included the LV free wall (n=8) and the RV free wall (n=2). In one procedure, both LV and RV free wall ablations were performed at apical sites. Steam pops occurred in two LV free wall cases, both without effusion. No other complications occurred. Over a 7-month follow-up (IQR 5–14), two patients (three procedures) had recurrence of VT.
Conclusion
Bipolar endo-epicardial catheter ablation is a feasible, safe, and effective option for patients with structural heart disease and deep intramural scars. It may be considered the treatment of choice when unipolar ablation is ineffective. Additional unipolar lesions were often applied to optimize lesion depth.