Background:Patients with atrial fibrillation (AF) and liver cirrhosis present a complex therapeutic dilemma, balancing elevated thromboembolic risk against substantial bleeding hazards. Comparative data on LAAO versus oral anticoagulation (OAC) in cirrhotic patients are lacking.
Methods: We analyzed patients encountered from 2011 – 2024 with non-valvular AF and liver cirrhosis in the TriNetX global research network. Individuals undergoing LAAO were propensity-score matched 1:1 to patients on OAC based on age, sex, and relevant comorbidities (e.g., hypertension, diabetes, heart failure, coronary heart disease, prior stroke, peripheral artery disease, chronic kidney disease, alcohol abuse, baseline hemoglobin). After matching, 1,681 patients remained in each group. Median follow-up duration was 449 days in the LAAO group and 430 days in the OAC group. Outcome analyses were uniformly truncated at 24 months post index event ensuring balanced comparability. The primary endpoint was a composite net clinical benefit, defined as the occurrence of stroke (ischemic or hemorrhagic), systemic arterial embolism, transfusion, or death.
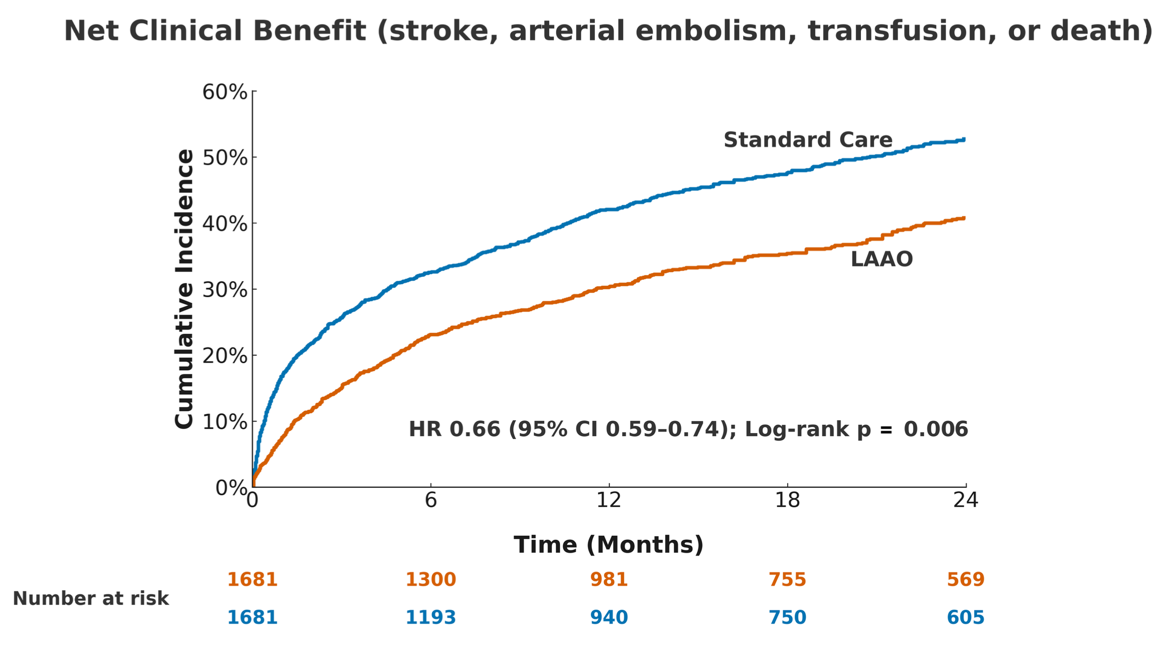
Results: The net clinical benefit composite occurred significantly less often in the LAAO group (537 vs. 745 events; HR 0.66, 95% CI 0.59–0.74; p=0.006). LAAO was associated with a lower risk of all-cause mortality (HR 0.55, 95% CI 0.48–0.64; p<0.0001; 298 vs. 504 deaths), stroke or intracranial bleeding (HR 0.77, 95% CI 0.63–0.94; p=0.010; 182 vs. 222 events), and arterial embolism (HR 0.46, 95% CI 0.26–0.79; p=0.004; 19 vs. 40 events). Transfusion events were numerically lower with LAAO but did not reach statistical significance (HR 0.86, 95% CI 0.70–1.05; p=0.42; 172 vs. 192 events).
Conclusion: Among patients with AF and liver cirrhosis, LAAO was associated with a significantly improved net clinical benefit compared to OAC. These findings support LAAO as a safe and potentially more effective alternative in this population