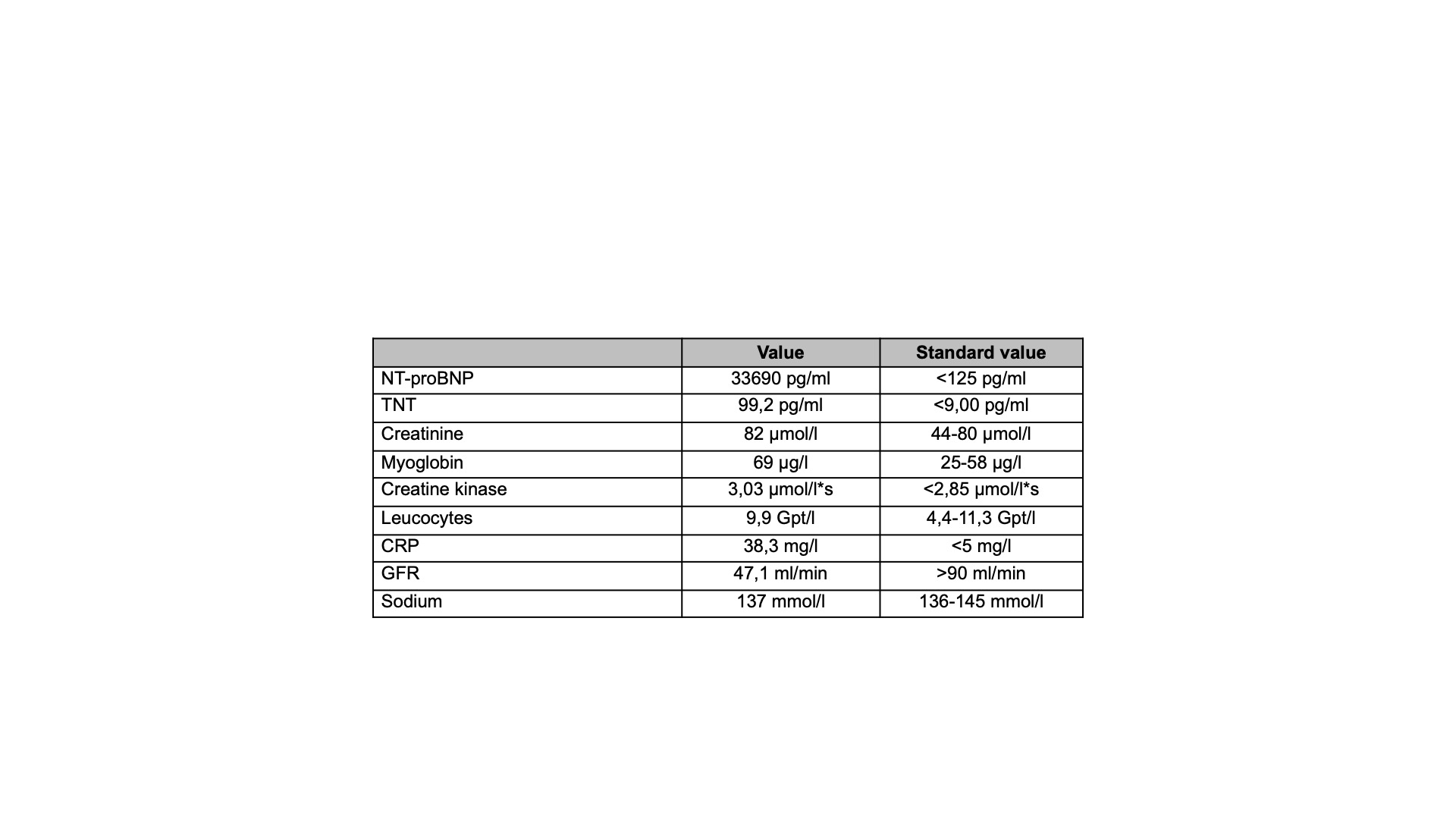
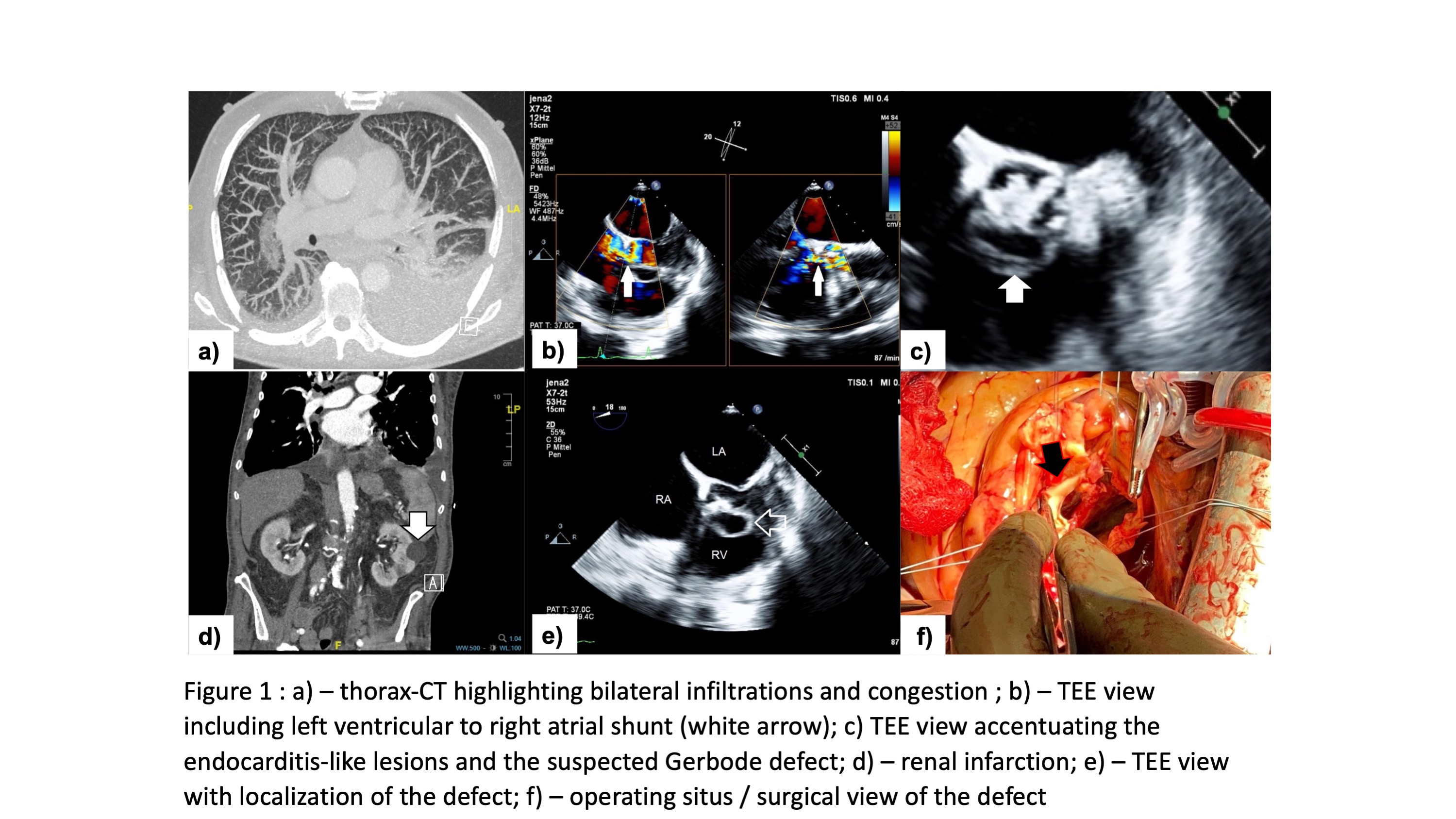
Background: Left ventricular to right atrial shunt (“Gerbode defect”) is an anatomical pathology in membranous septum following communication between left ventricle and right atrium. Its origin is mainly congenital, but very rarely this defect is acquired due to trauma, infectious endocarditis, myocardial infarction, valve replacement and septal surgery. Aim / Purpose: Through this case report we want to present a very rare case of acute heart failure caused by a left ventricular to right atrial shunt in infectious endocarditisPresentation and primary Investigations: A 70-year-old man presented to our heart failure unit with dyspnea (NYHA IV), deteriorating general condition and shock constellation. Previously a PCI of the RCA was performed due to NSTEMI. His medical history consisted of chronic coronary disease, severe aortic and mitral valve insufficiency, renal infarction, and insufficiency. Furthermore, the patient suffered recently from infections of urinary tract. The ECG showed a sinus tachykardia and no signs of acute ischemia. The blood tests are shown in Table 1. The physical exam presented clinical signs of volume overload such as peripheral oedema, elevated jugular vein pulse and gallop sounds in the auscultation Imaging: A CT-Examination demonstrated signs of congestion and bilateral infiltrates and a left renal infarction. Transthoracic echocardiogram was performed for further delineation of cardiac structural abnormalities. Biventricular systolic function was preserved. Severe aortic and mitral regurgitation were identified. In the transesophageal echocardiogram a left ventricular to right atrial shunt was detected. Furthermore, endocarditis-like lesions of all aortic cusps were depicted.Treatment: Following heart team consultation in the echocardiogram lab, the patient was immediately accompanied in the operating room and an aortic and mitral valve replacement as well as reconstruction of the atrioventricular situs was performed. The postoperative phase was characterized by progressive septic shock and the patient passed away on the first postoperative day.Conclusion: Through this case report we would like to raise awareness toward a rare entity of acute heart failure such as left ventricular to atrial shunt or acquired Gerbode defect. It represents a condition with high morbidity and mortality and should be immediately referred to a tertiary heart centre with multidisciplinary teams composed by cardiologists, cardiac surgeons, infectious disease and intensive care specialists.