Background: Transoesophageal echocardiography (TEE) is essential for guiding transcatheter tricuspid edge-to-edge repair (T-TEER); however, mucosal injury of the oesophagus and stomach remains an emerging safety concern. Systematic correlation between peri-procedural endoscopic findings and right-heart haemodynamics during T-TEER has not been reported.
Methods: We prospectively analysed 100 consecutive patients with severe tricuspid regurgitation undergoing T-TEER (TriClip or PASCAL) at the University Hospital Heart Centre Brandenburg between November 2020 and April 2024. All patients underwent standardized esophagogastroduodenoscopy before and after the procedure. Injuries were mapped according to distance from dental row. Haemodynamic data were obtained from pre-procedural right-heart catheterization (RHC). Two models were evaluated: (1) compared any mucosal injury versus no injury; (2) examined clinically relevant (Grade 4) injuries requiring haemoclips versus all others.
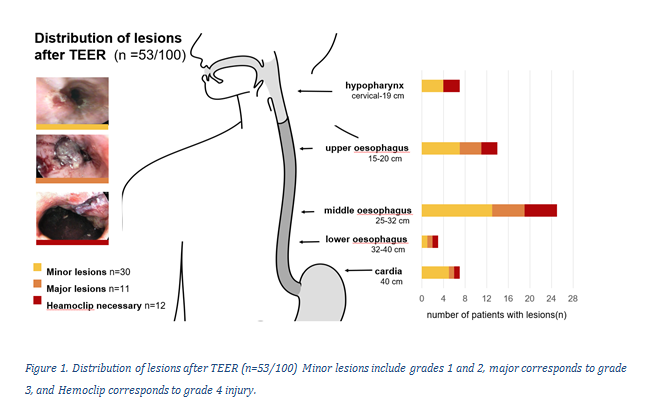
Results: New post-procedural mucosal injuries occurred in 53% of patients (Figure 1), predominantly at the mid-oesophagus (25–35 cm from the dental row). Procedural characteristics, including probe manipulation and duration, did not differ between groups. Clinically relevant injuries were associated with higher right-sided pressures: mean pulmonary artery pressure (33 ± 7 mmHg vs. 26 ± 6 mmHg; p=0.019), pulmonary capillary wedge pressure (22 ± 5 mmHg vs. 19 ± 4 mmHg; p=0.025) and inferior vena cava diameter (27 ± 5 mm vs. 23 ± 4 mm; p=0.028). Pulmonary capillary wedge pressure independently predicted both, clinically relevant injury (Exp(B) 1.153 [95%CI 1.034-1.286], p=0.010) and 3-month mortality (Exp(B) 1.132 [95%CI 1.1018-1.258], p=0.022).
Conclusions: TEE-related oesophageal and gastric injuries are common during T-TEER and show a distinct anatomical pattern. Elevated PCWP may increase susceptibility to TEE-related oesophageal injury through venous congestion and mucosal edema, highlighting the need for haemodynamic risk assessment before T-TEER.