Background:
Left bundle branch area pacing (LBBAP) is a promising physiological pacing technique but remains technically demanding. Data on learning curves and their impact on procedural outcomes are limited.
Purpose:
To evaluate the learning curve for LBBAP implantation with respect to procedural success, radiation exposure and procedure duration over consecutive implantations.
Methods:
LBBAP implantations at a single centre were retrospectively analysed. Success was defined as confirmed left bundle branch area capture on ECG as follows: QRS morphology transition during threshold testing, r-prime in V1, V6RWPT <90ms and V6-V1 interpeak interval >40ms. Procedural parameters included success rate, radiation dose, and procedure duration. Logistic regression and temporal trend analysis were used to evaluate changes in performance over time.
Results:
Eighty (n = 80) patients (mean age 75.5 ± 10.6 years; mean BMI 27.7 ± 5.1 kg/m²; 75.0% male) with a mean LVEF of 36.4 ± 8.4% and a baseline QRS duration averaged 153.9 ± 23.1 ms were included (n = 46 lumenless leads, n = 34 stylet-driven leads) including them being new implantations (n = 39) and upgrades (n = 41). There were two operators involved in the study, operator A (OP-A) with 61 (76.3%) cases, operator B (OP-B) 19 (23.7%) cases.
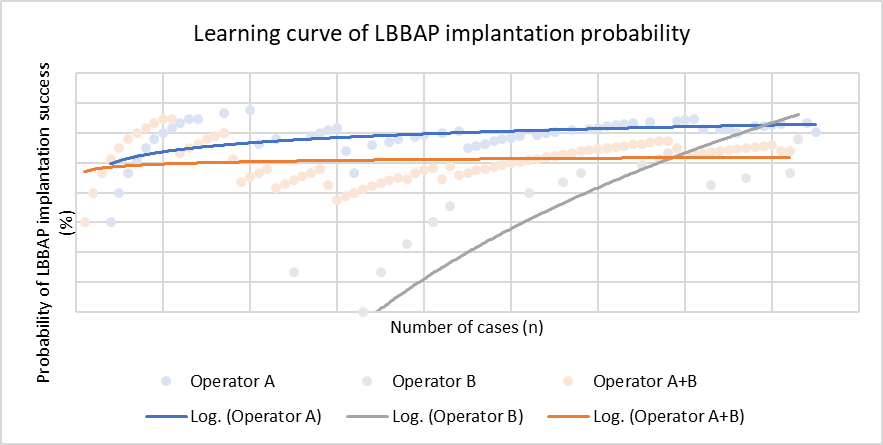
Learning curve modelling showed an increase in implantation success during the early phase (Figure 1), recognising that operators did not start from zero experience. When combining both operators, a plateau was observed after approximately 60–70 cases, with a probability of successful implantation of 82.8% after one third of cases and 86.3% after 80 cases. OP-A exhibited a steeper learning curve with an indication of plateau formation towards the end of the cohort, reaching 88.2% success after one third of cases and 90.3% after 61 cases. OP-B showed a continuously rising curve without reaching a plateau in this dataset, with success rates of 71.4% after one third and 88.9% after 19 implantations. Mean implantation duration for OP-A after one half of implantations was 108.7 ± 24.7min; after 61 cases 99.8 ± 26.1min, while remaining stable and shorter (79.5 ± 28.0min) for OP-B. Mean implantation duration decreased with both groups combined from 100.7 ± 32.0 min to 93.8 ± 28.0 min. No temporal trend was observed in radiation dosage. A plateau was reached early in the stylet-driven leads (20-30 cases) compared to the lumenless leads which did not reach a plateau yet in this cohort.
Conclusions:
LBBAP shows a clear learning curve with improving success rates and shorter procedure duration over time. A performance plateau was reached after approximately 60–70 cases. Stylet-driven leads demonstrated a faster learning curve than lumenless systems. Factors influencing the learning curve may include technical advancement, patient selection, differences between primary implantations and upgrades, and the overall sample size. These findings highlight the importance of growing operator experience to achieve optimal LBBAP outcome.