Background:
Monitoring left ventricular filling pressure (LVFP) in ambulatory patients with heart failure (HF) improves outcomes, but currently available devices are invasive, expensive and require life-long antithrombotic therapy. Seerlinq is a CE-certified (MDR class IIb), non-invasive system for remote LVFP monitoring, utilizing advanced photoplethysmographic (PPG) signal analysis based on artificial intelligence and hemodynamic principles.
Purpose:
To evaluate the effect of the Seerlinq system on HF hospitalization (HFH) and mortality rates in a real-world HF outpatient population.
Methods:
STOP-DHF (Strategy TO Prevent Decompensated HF) is a multi-center, prospective, single-arm, open-label trial with a prespecified effectiveness endpoint. The study enrolled HF patients in NYHA functional class II and III, regardless of ejection fraction. This predefined subgroup analysis focused on patients with HFH within the past 12 months prior to enrolment. Patients performed 2 PPG measurements using a standard pulse oximeter connected to a smartphone, one while calmly standing and the second in a recumbent position every other day. Together with each measurement, patients entered blood pressure values from home BP monitor and reported their symptoms (shortness of breath and fatigue) in the study application. Data were uploaded remotely and analyzed using the Seerlinq system.
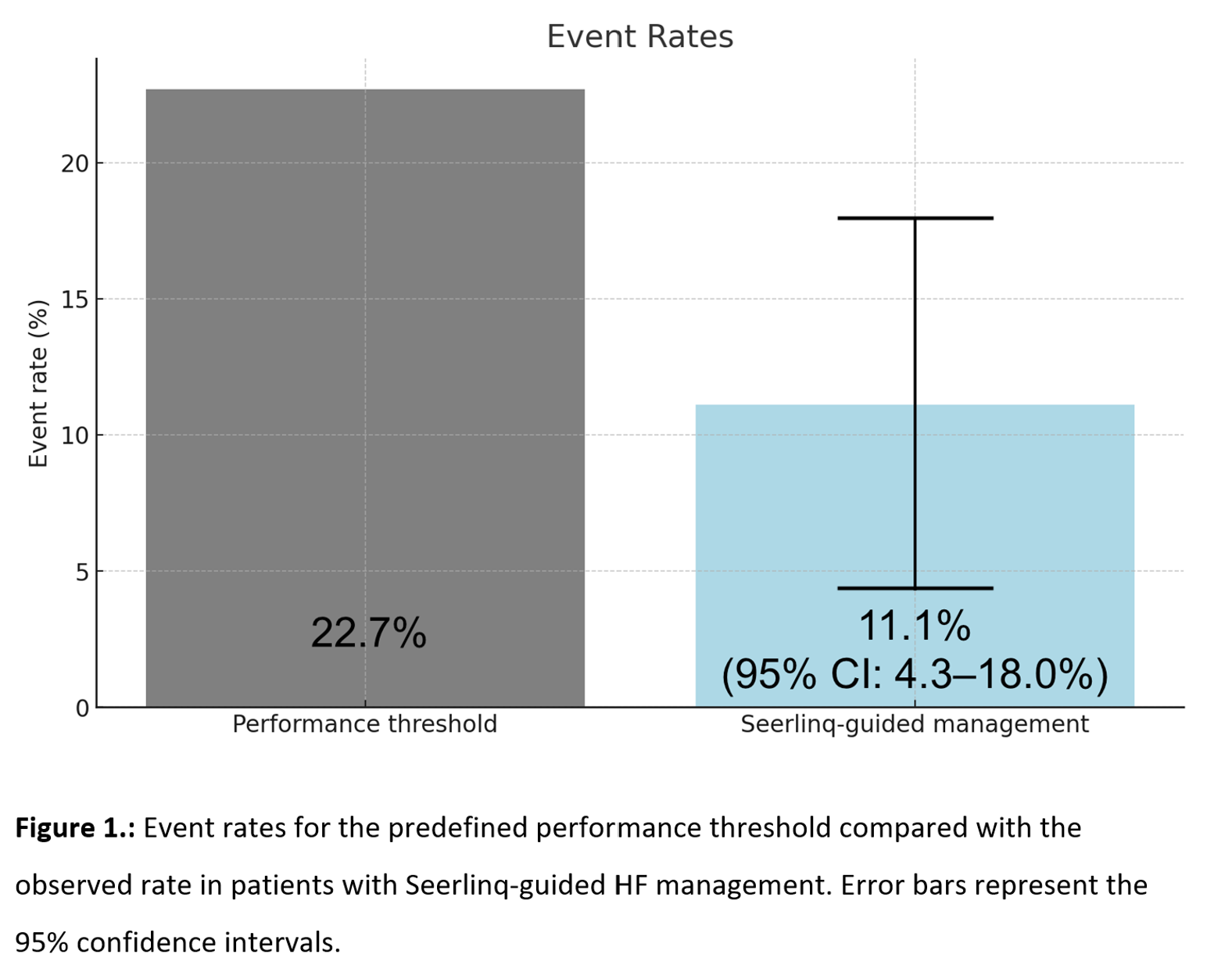
The clinical outcome was defined as the composite of HFH and all-cause mortality at 6 months. The performance goal was determined based on local epidemiological data (22.7%).
Results:
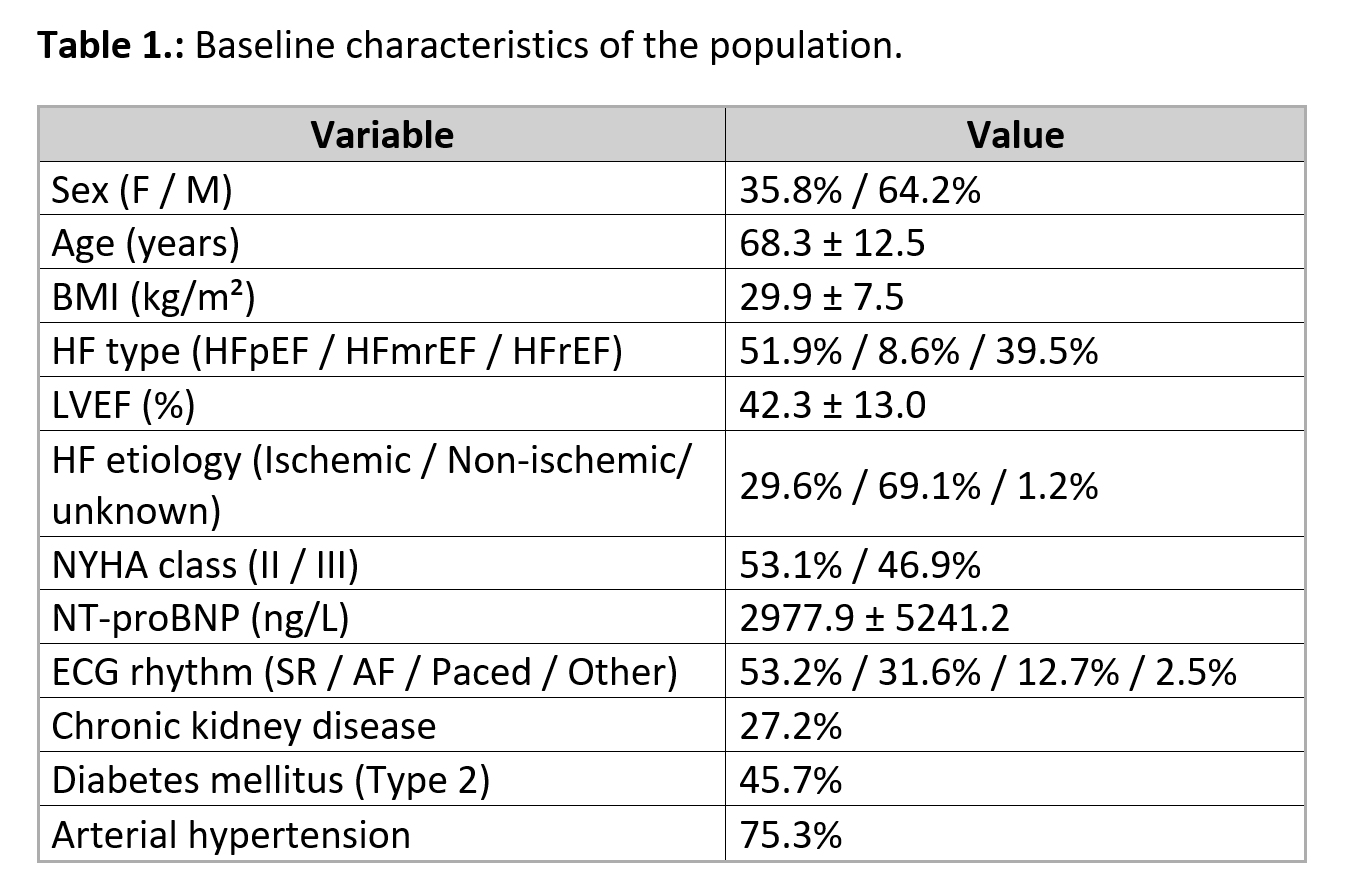
From a total of 310 HF patients enrolled between November 2023 and May 2025 (Table 1), 81 patients with prior HFH were included in this subanalysis (mean age 68.6±12.2 years, 33% female, 54% HFrEF, 7% HFmrEF, 38% HFpEF, NYHA II: 53%, NYHA III: 47%). The composite primary outcome was significantly lower (Figure 1) in the Seerlinq-guided group compared with the prespecified performance goal (11.1% vs. 22.7%, 95% CI 4.3–18.0%, p=0.0061). The individual components were: HFH rate of 2.47% (2/81) and all-cause mortality of 8.64% (7/81).
In the entire STOP-DHF cohort of NYHA II and III patients (including those without recent HFH), the event rate was 4.52% (95% CI: 2.2–6.8%).
Conclusion:
In HF patients recently hospitalized for decompensation, non-invasive, remote LVFP monitoring with the Seerlinq system was associated with substantially lower rates of HFH or mortality compared to epidemiological expectations. These results suggest that Seerlinq-based LVFP monitoring may provide a scalable, non-invasive alternative to current invasive monitoring systems.



