Background: Cardiogenic shock (CS) is a complex syndrome with a high mortality rate exceeding 40%. Emerging evidence suggests sex-related differences in presentation, management and outcomes. This study aims to investigate differences in early lactate dynamics and outcome prediction by sex in CS.
Methods: We analyzed 591 CS patients from the multicenter MIRACLE cohort, including prospective cases from August 2024 and retrospective cases from 2018–2023 at University Hospital Freiburg. Patients with SCAI A or non-cardiac shock triggers were excluded, leading to a cohort of 471 patients. Lactate trajectories during the first 4 and 8 hours were classified as Clearance (≥50% decrease or lactate <2 mmol/L), Partial Clearance (10–50% decrease), or No Clearance (<10% decrease). Sex-specific survival analyses were performed using Kaplan–Meier curves and Cox proportional hazards models across lactate trajectories as well as baseline lactate, adjusting for age and prior cardiac arrest. Interaction terms were used to evaluate sex differences in lactate trajectory and their association with 30-day mortality.
Results: Among 471 patients included in the analysis, 141 were women (29.9%). Women were older and less often presented with AMI-related shock, while men had higher rates of prior myocardial infarction and cardiac arrest. SCAI stage, baseline lactate, and 30-day mortality were similar between sexes.
Early lactate trajectories were strongly associated with 30-day mortality in the overall cohort. At 8 hours, “No Clearance” was linked to substantially higher mortality (HR 2.81, 95% CI 1.46–5.39, p = 0.0019). Sex-stratified models showed comparable effect sizes in women and men (Figure 1), although confidence intervals were wider in women due to smaller sample size. Interaction testing demonstrated no evidence of sex-specific modification of the lactate–mortality relationship (LRT p≈0.27), indicating similar prognostic value of lactate clearance across sexes. Kaplan-Meier curves indicate higher mortality rates in those without Lactate Clearance for both sexes (Figure 2).
Conclusion: Women with cardiogenic shock were older but showed comparable 30-day mortality and received similar treatment intensity. These preliminary results indicate comparable prognostic value of early lactate trajectories between genders, yet bigger cohorts are needed for further validation and may improve early, individualized risk stratification.
Baseline characteristics (male vs. female):
Age (median [Q1–Q3]): 68.2 [59.2–78.0] vs. 75.2 [64.7–82.2], p = 0.001.
Type of CS: AMI-CS 63.0 % vs. 51.1 %, ADHF-CS 20.0 % vs. 28.4 %, Secondary-CS 13.6 % vs. 14.9 %, p = 0.069.
SCAI class: B 35.2 % vs. 36.2 %, C 20.9 % vs. 17.7 %, D 26.1 % vs. 30.5 %, E 17.9 % vs. 15.6 %, p = 0.705.
Cardiac arrest prior to ICU: 32.4 % vs. 23.4 %, p = 0.061.
Prior myocardial infarction: 23.0 % vs. 12.1 %, p = 0.005.
Admission lactate (mmol/L, median [Q1–Q3]): 3.20 [2.20–6.00] vs. 3.80 [2.20–6.60], p = 0.265.
30-day mortality: 36.1 % vs. 36.2 %, p = 1.000.
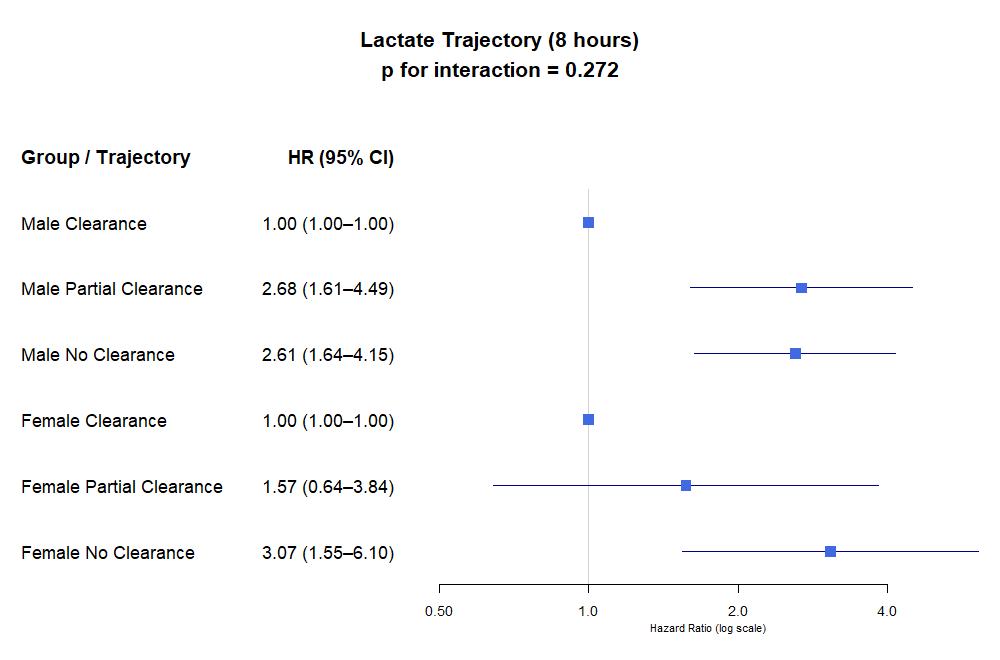
Figure 1: Lactate trajectory within 8 hours after admission stratified by sex.
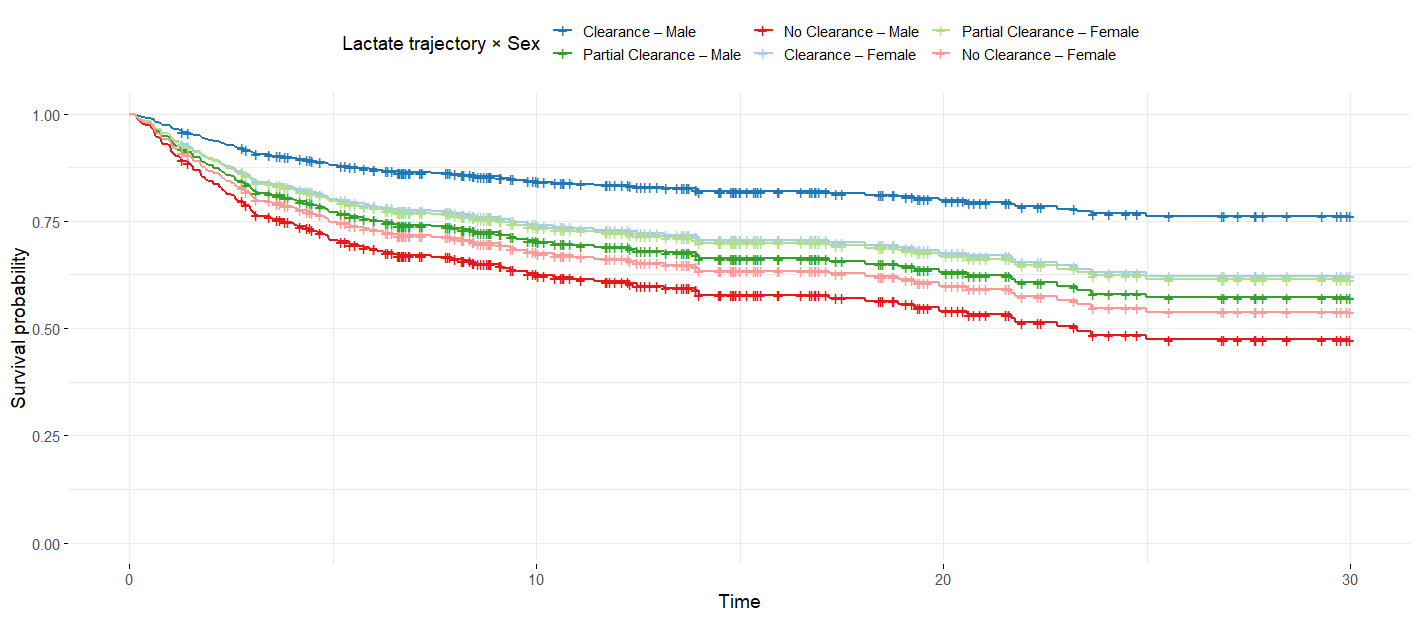
Figure 2: Kaplan-Meier survival curves by lactate trajectory and sex.



