Introduction:
Pulsed Field Ablation (PFA) of atrial fibrillation (AF) is a rapidly expanding ablation method and is believed to lower overall complications. However, the rate of cerebrovascular complications seems to vary considerably between catheter systems and mechanisms leading to cerebral embolization and microemboli formation are still unclear:
This study was designed to investigate the effect on enhanced catheter flushing and ablation location on cerebral embolization during AF ablation using a variable loop circular catheter (VLCC).
Methods:
Consecutive patients who presented for first-time atrial fibrillation ablation using a VLCC were prospectively recruited at DHZC, Campus Benjamin Franklin. After the first 11 patients, irrigation rate was elevated from 4 ml/min to 30ml/min according to a change in the manufacturer’s recommendations.
Transcranial doppler (TCD) was used to detect microembolic signals (MES) and was used throughout the entire procedure. MES were assigned to each procedural step and ablation pulse; each detected MES was manually controlled by a neurologist after the procedure was completed.
Additionally, cerebral MRI was performed within 24 hours after ablation to detect acute cerebral infarction. Silent cerebral lesions (SCL) were defined as lesions with high diffusion weighted imaging signal and low apparent diffusion coefficient signal. Clinical examination was performed within 24 hours after ablation using the National Institutes of Health Stroke Scale (NIHSS).
Results:
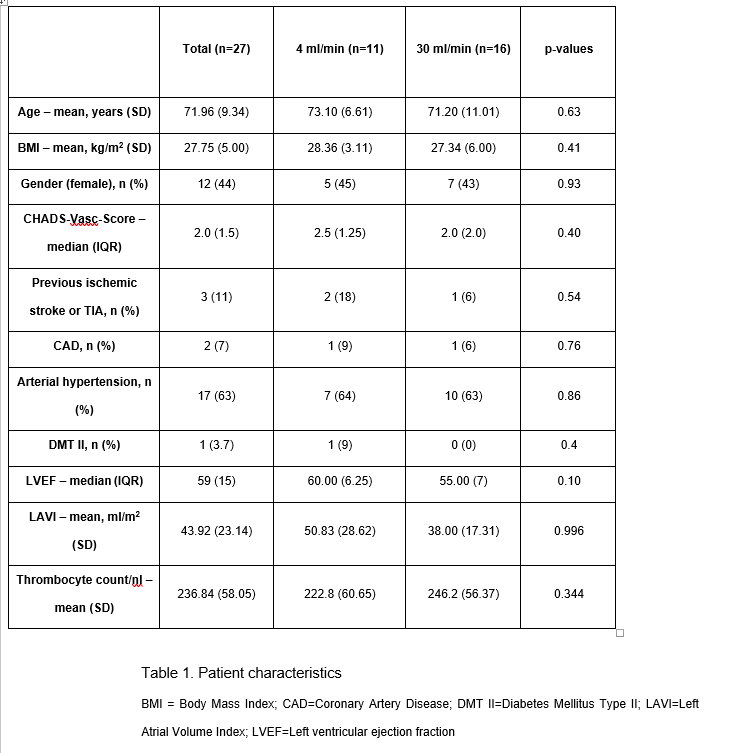
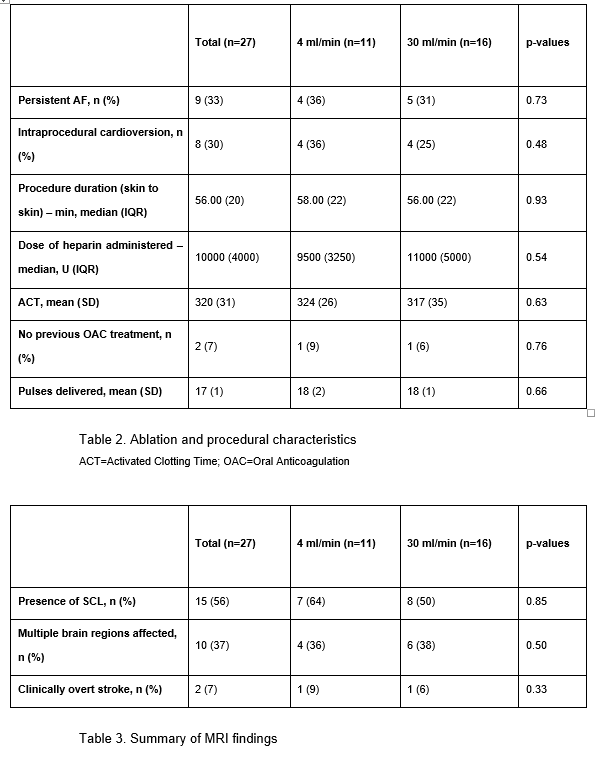
25 patients were included. Catheter ablation was successfully performed with single transseptal puncture in all patients. There were no clinical baseline differences between the two groups (see table 1). Additionally, ablation time, mean ACT, heparin dose and delivered pulses were similar (see table 2).
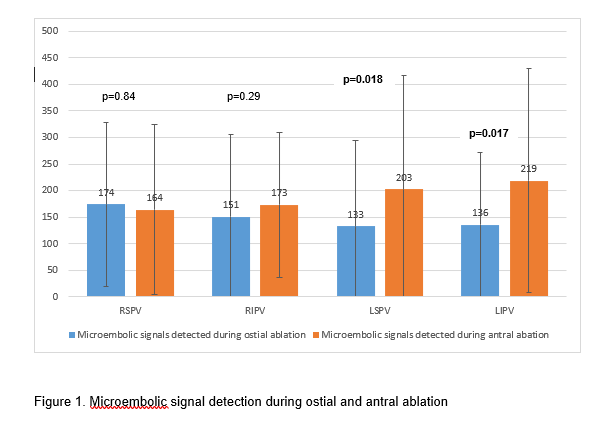
MES count did not significantly differ between the two groups (4 ml irrigation rate: 1046+677 vs. 30 ml irrigation rate:1881+1208, p=0.065). SCL were detected by MRI in 15 (56%) patients with no differences between the two groups (see table 3). Of those, two patients (one in each group) reported new focal neurological deficits. Both patients had a NIHSS score of 1. Symptoms resolved within one week in one patient and persisted in the other. The presence of SCL was not associated with elevated MES count (1515+1107 for the group without cerebral lesions vs. 1526+1028 for the group with silent lesions, p=0.98). MES detection was highest during antral ablation of the left-sided pulmonary veins (see figure 1).
Conclusion:
This study confirms the results of previously published data indicating a high number of postprocedural SCL as well as microembolic signals detected during ablation using a VLCC. Despite experimental data indicating a favourable safety profile, enhanced irrigation rate in ablation was not associated with lower cerebral microembolism. Catheter design, the influence of catheter-tissue contact and energy output should be further investigated to identify potential drivers to reduce cerebral microembolisms.