Background
Pulsed-field ablation (PFA) provides tissue-selective myocardial ablation with a favourable collateral safety profile compared to thermal techniques. Meanwhile, radiofrequency (RF) is well established and extensively studied for lesion creation and durability. A new dual-energy, contact-force catheter integrated with a 3D electroanatomic mapping system enables switching between RF and PFA within a single workflow, aiming to utilise the complementary strengths of both energies. RF is used where durability is essential (such as anterior, ridge, or carina regions), while PFA is employed where collateral safety is the priority (posterior or inferior areas). Limited real-world data exist on the performance and safety of this hybrid approach, highlighting the need for focused evaluation.
Methods
Consecutive patients with atrial fibrillation (AF) undergoing their first pulmonary vein isolation (PVI) were included. PVI was performed with focal ablation, creating contiguous wide-antral encirclement of ipsilateral pulmonary veins using a contact-force (CF) sensing Dual-energy THERMOCOOL SMARTTOUCH SF (DE STSF) catheter (Biosense Webster, Inc.). Pulsed-field ablation (PFA) was applied to posterior and inferior segments with a target pulsed field index (PFI) of 400, and radiofrequency (RF) to anterior, ridge, and carina segments with a target AI of 550. Venous blood samples were obtained before and after the procedure to evaluate parameters related to intravascular haemolysis (IH). Severe haemolysis was defined in accordance with the current haematological guidelines as free haemoglobin greater than 100 mg/l. Oesophageal endoscopy was performed within one to three days. The majority of patients underwent cerebral MRI to screen for silent cerebral lesions.
Results
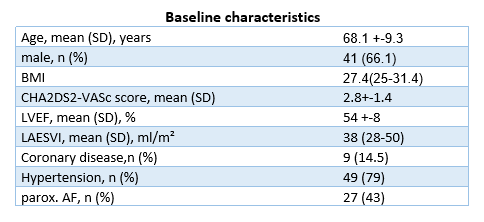
Altogether, 62 consecutive patients undergoing their first AF procedure were included (average age 68.1 ± 9.3 years; 41 (66.1%) male; CHA₂DS₂-VASc score 2.8 ± 1.4; 27 (43%) with paroxysmal AF). The median procedural duration was 91.0 (79.0–114.2) minutes, with a total effective ablation delivery time of 21.0 (18.0–26.0) minutes. The number of applications per case was 63.0 (40.0–84.5) for RF and 42.7 (32.0–65.0) for PF.
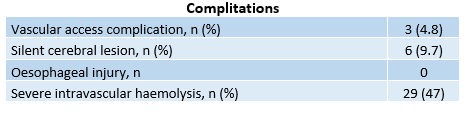
An endoscopic examination was performed in all patients, with no oesophageal injuries detected. Cerebral MRI was obtained in 75% of the patients; among those scanned, 6 (13%) had clinically silent acute ischemic lesions. Three patients experienced vascular complications (aneurysma spurium) all of which were successfully managed with conservative treatment.
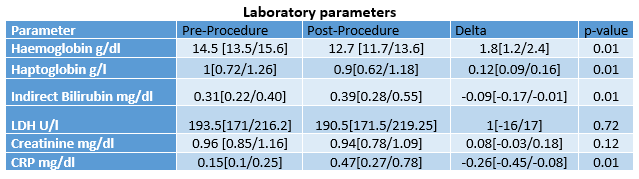
Regarding haemolysis, the overall incidence of haematologically defined severe intravascular haemolysis (free haemoglobin >100 mg/L) was observed in 29 (47%) patients. There was a statistically significant decrease in haemoglobin levels after the procedure, with a mean reduction of 1.8 g/dL. Overall, there was no significant change in serum creatinine levels before and after the ablation. Only one patient developed acute kidney injury, defined as an increase in serum creatinine of more than 0.3 mg/dL.
Conclusion
Dual-energy ablation demonstrates procedural feasibility with short procedure times and a favourable safety profile. No oesophageal injury was documented, and the rate of silent cerebral lesions was in line with previously reported data. Although intravascular haemolysis was frequent, it remained without significant clinical consequences.