Background
Heart failure (HF) is a chronic, progressive condition with high morbidity and mortality. Clinical identification and diagnosis of HF is challenging since symptoms are often nonspecific, patients present with multiple comorbidities, and the underlying disease causes can overlap. Left ventricular ejection fraction (LVEF) is a crucial tool to identify and define HF with reduced LVEF (HFrEF), with mildly reduced LVEF (HFmrEF), or HF with preserved ejection fraction (HFpEF). To estimate public health impact of HF and its subtypes in Germany, population-level data that cover a broad age range are needed. Magnetic resonance imaging (MRI) has the potential to provide a robust and reproducible definition of HF.
Methods
We analyzed N=28’394 individuals from the population-based, prospective, multi-center NAKO health study representing 16 study regions in Germany, who underwent whole-body magnetic resonance imaging. LVEF and LV mass were obtained from short-axis cine images and LV Mass Index (LVMI) was calculated as end-diastolic mass divided by body surface area (duBois formula). HFrEF was defined as LVEF ≤40%, HFmrEF as LVEF >40%, but <50%, and HFpEF as LVEF ≥50% with LVMI ≥65.4 g/m2 (women) or ≥84 g/m2 (men), with the cutoffs corresponding to the 97.5% percentile of mass distribution of the whole sample. Self-reported physician diagnosis of HF was ascertained by questionnaire. Statistical survey weights accounting for sampling design and relevant sociodemographic factors were used to calculate population prevalences for HF and its subtypes in the NAKO study regions.
Results
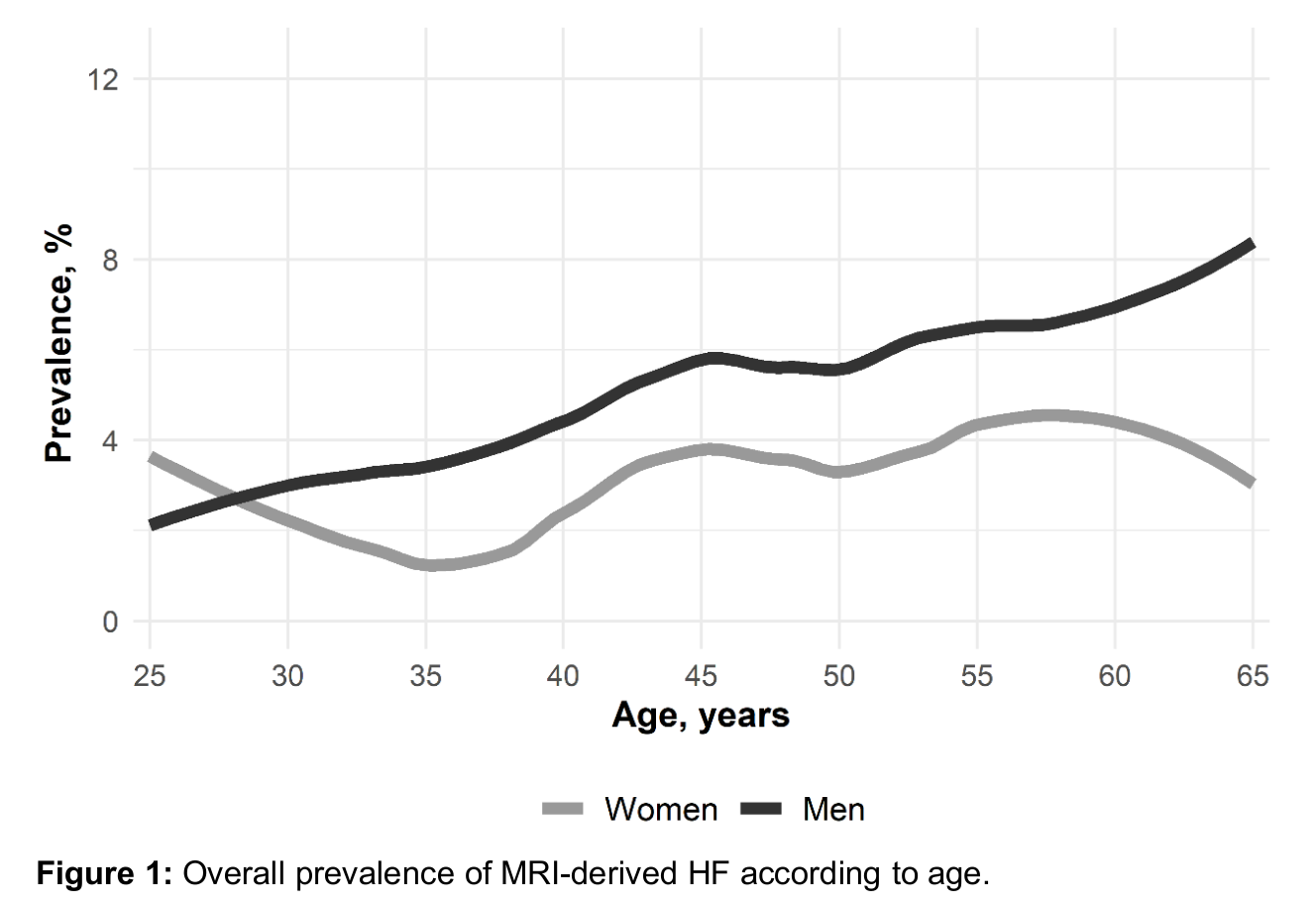
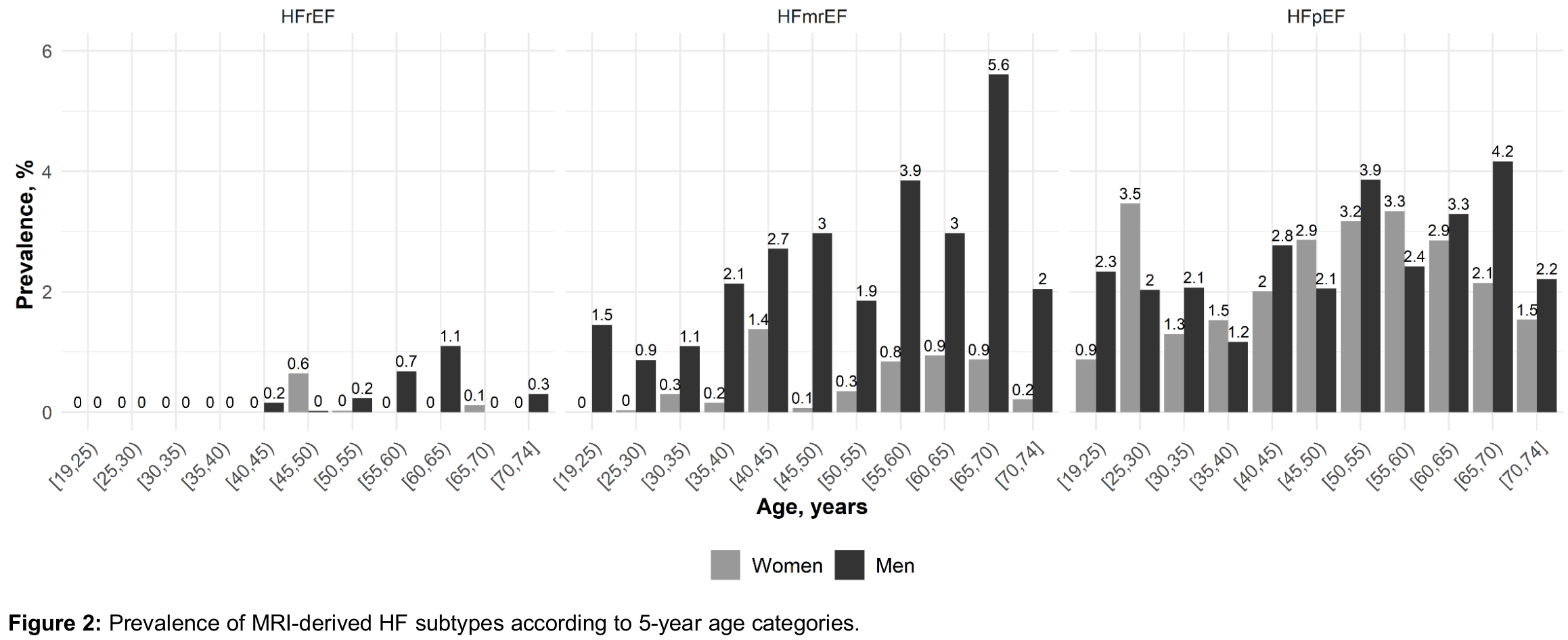
The weighted sample comprised 50.6% women and had a mean age of 45.5 years (standard deviation 13.9 yrs). The overall prevalence of MRI-derived HF was 4.1% (3.0% in women, 5.3% in men) with substantial age dependency (Figure 1). In women, HFpEF and HFmrEF accounted for 81.1% and 16.1% of all HF cases, respectively. In men, HFpEF and HFmrEF accounted for 49.5% and 46.5% of all HF cases, respectively. For any HF subtype, prevalence showed non-linear dependency on age (Figure 2). The overall prevalence of self-reported HF diagnosis was 1.8% (1.8% in women, 1.7% in men). Of those with any MRI-derived HF, the proportion who had a self-reported diagnosis was 6.6% (8.1% in women, 5.6% in men). Average LVEF in % was 34.9 (standard deviation 3.4), 46.9 (2.8), and 62.9 (5.5) in individuals with MRI-derived HFrEF, HFmrEF and HFpEF, respectively, compared to an LVEF of 63.3 (5.1) in individuals without HF. Individuals with HFrEF were oldest with 54.5 (7.1) years, compared to 50.6 (12.6) for HFmrEF, 48.0 (13.5) for HFpEF, and 45.4 (13.9) for no HF. They had highest BMI with 29.8 (5.1) kg/m2, compared to 29.1 (5.7) for HFmrEF, 26.4 (4.8) for HFpEF and 26.6 (5.2) for no HF, and highest values of systolic blood pressure with 140.7 (21.4) mmHg, compared to 135.3 (19.0) for HFmrEF, 138.7 (21.6) for HFpEF and 126.0 (15.6) for no HF.
Conclusion
Representative for a major part of the German population, prevalence of MRI-derived HF was high and substantially exceeded self-reported prevalence in the population-based NAKO health study. This underscores not only the considerable public health relevance of HF but also the potential diagnostic gap in current clinical practice. Further, our results emphasize the utility of MRI to ascertain clinically relevant manifestations of HF and its subtypes, and point to its potential to identify at-risk individuals.